

Extramural Venous Invasion and Tumor Deposit at Diffusion-weighted MRI in Patients after Neoadjuvant Treatment for Rectal Cancer
- PMID: 37581503
- PMCID: PMC10478788
- DOI: 10.1148/radiol.230079
Extramural Venous Invasion and Tumor Deposit at Diffusion-weighted MRI in Patients after Neoadjuvant Treatment for Rectal Cancer
Abstract
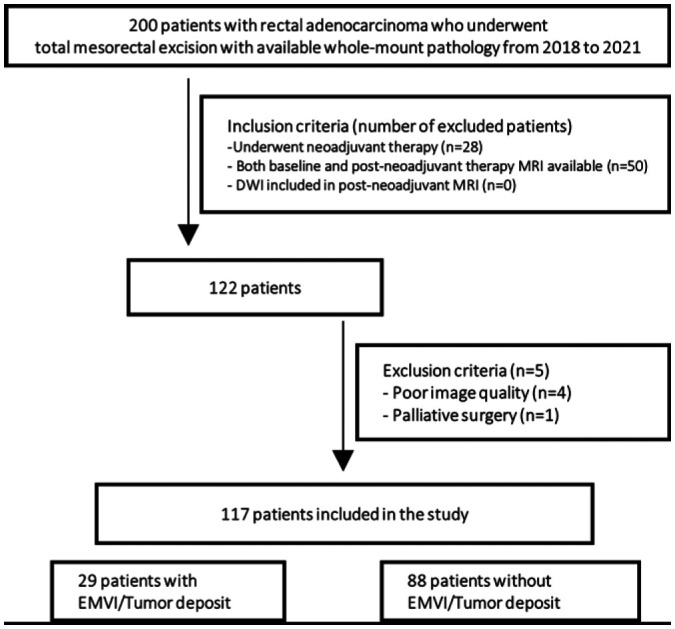
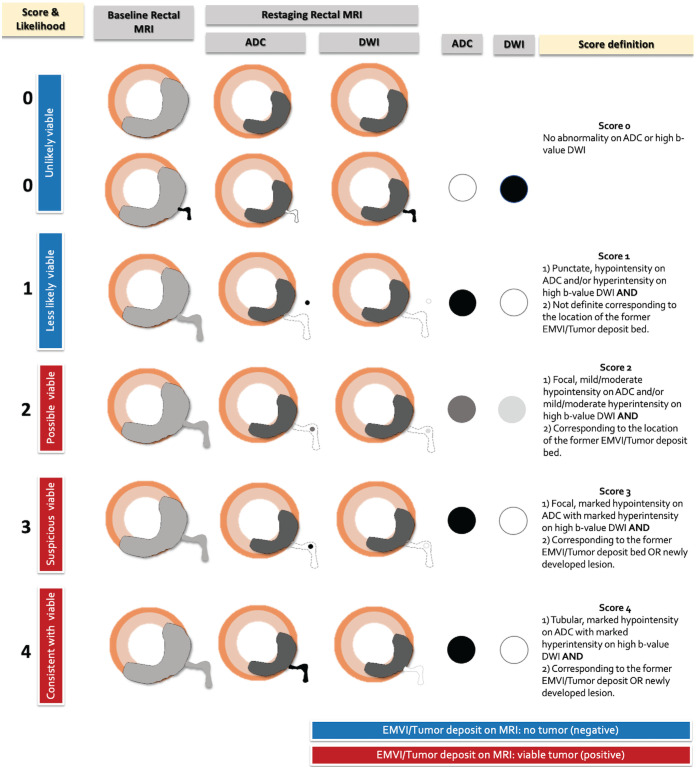
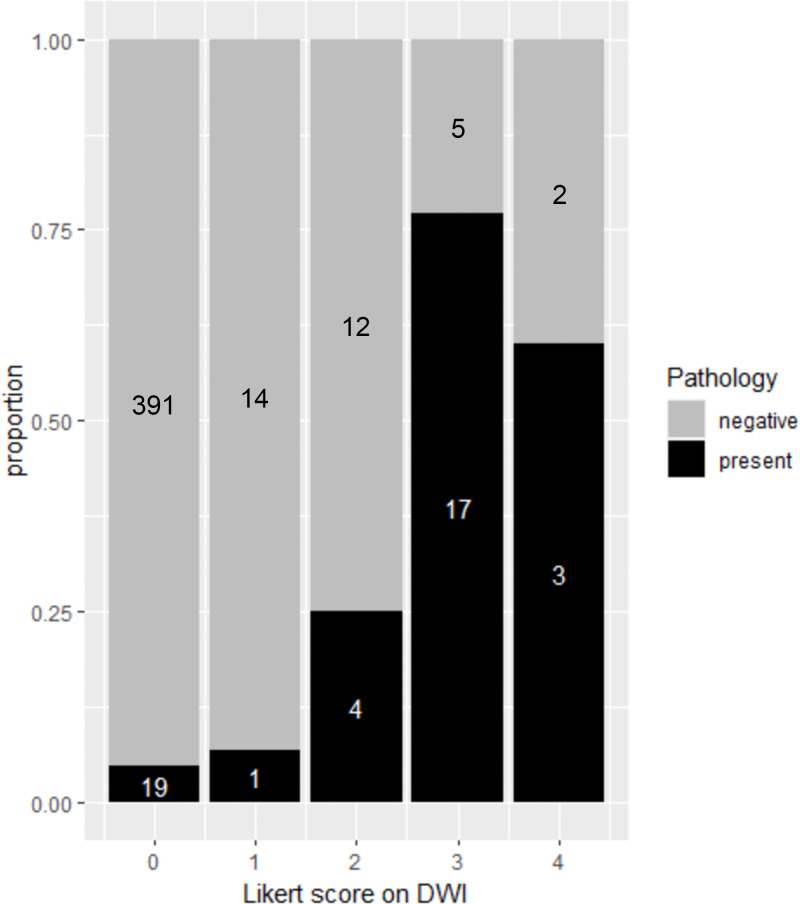
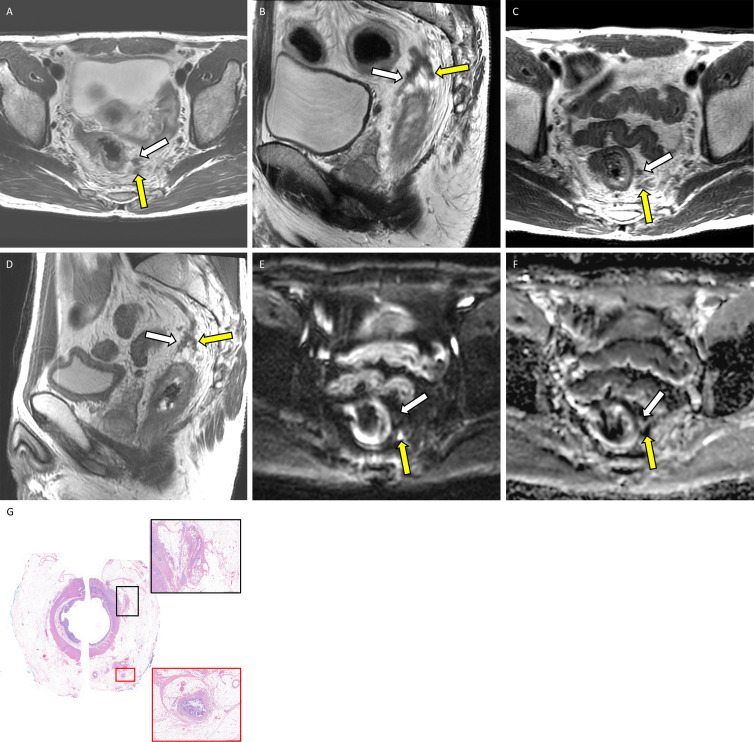
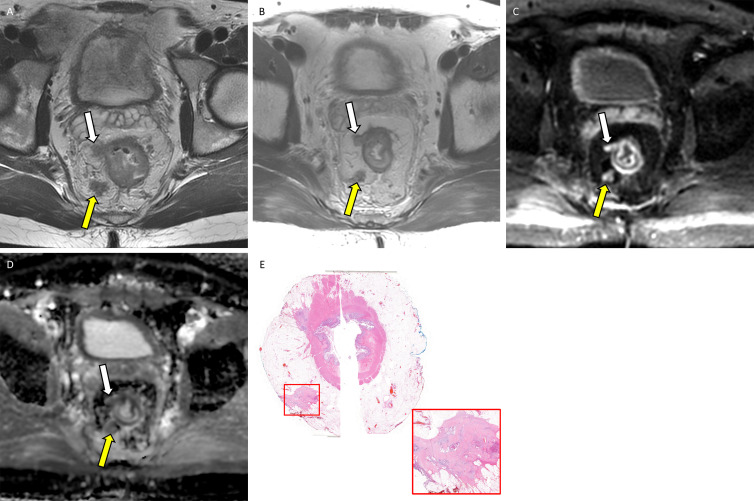
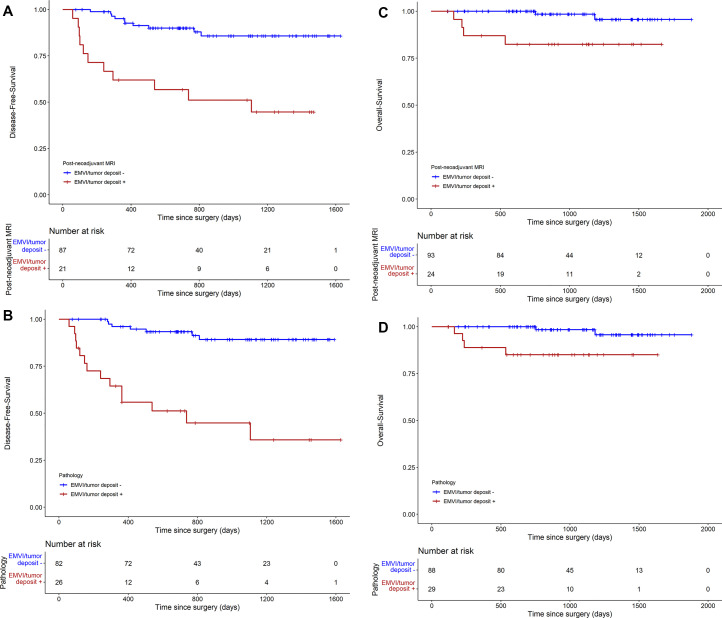
Background Diffusion-weighted (DW) imaging is useful in detecting tumor in the primary tumor bed in locally advanced rectal cancer (LARC) after neoadjuvant therapy, but its value in detecting extramural venous invasion (EMVI) and tumor deposit is not well validated. Purpose To evaluate diagnostic accuracy and association with patient prognosis of viable EMVI and tumor deposit on DW images in patients with LARC after neoadjuvant therapy using whole-mount pathology specimens. Materials and Methods This retrospective study included patients who underwent neoadjuvant therapy and surgery from 2018 to 2021. Innovative five-point Likert scale was used by two radiologists to independently evaluate the likelihood of viable EMVI and tumor deposit on restaging DW MRI scans in four axial quadrants (12 to 3 o'clock, 3 to 6 o'clock, 6 to 9 o'clock, and 9 to 12 o'clock). Diagnostic accuracy was assessed at both the per-quadrant and per-patient level, with whole-mount pathology as the reference standard. Weighted κ values for interreader agreement and Cox regression models for disease-free survival and overall survival analyses were used. Results A total of 117 patients (mean age, 56 years ± 12 [SD]; 70 male, 47 female) were included. Pathologically proven viable EMVI and tumor deposit was detected in 29 of 117 patients (25%) and in 44 of 468 quadrants (9.4%). Per-quadrant analyses showed an area under the receiver operating characteristics curve of 0.75 (95% CI: 0.68, 0.83), with sensitivity and specificity of 55% and 96%, respectively. Good interreader agreement was observed between the radiologists (κ = 0.62). Per-patient analysis showed sensitivity and specificity of 62% and 93%, respectively. The presence of EMVI and tumor deposit on restaging DW MRI scans was associated with worse disease-free survival (hazard ratio [HR], 5.6; 95% CI: 2.4, 13.3) and overall survival (HR, 8.9; 95% CI: 1.6, 48.5). Conclusion DW imaging using the five-point Likert scale showed high specificity and moderate sensitivity in the detection of viable extramural venous invasion and tumor deposits in LARC after neoadjuvant therapy, and its presence on restaging DW MRI scans is associated with worse prognosis. Published under a CC BY 4.0 license. Supplemental material is available for this article. See also the editorial by Méndez and Ayuso in this issue.
Conflict of interest statement
Figures
Comment in
-
Diffusion-weighted MRI for Diagnosing Extramural Venous Invasion in Rectal Cancer after Neoadjuvant Therapy: A Prognostic Biomarker.Radiology. 2023 Aug;308(2):e231661. doi: 10.1148/radiol.231661. Radiology. 2023. PMID: 37581500 No abstract available.
References
-
- Lord AC , D’Souza N , Shaw A , et al . MRI-Diagnosed Tumor Deposits and EMVI Status Have Superior Prognostic Accuracy to Current Clinical TNM Staging in Rectal Cancer . Ann Surg 2022. ; 276 ( 2 ): 334 – 344 . - PubMed
-
- Schaap DP , Voogt ELK , Burger JWA , et al . Prognostic Implications of MRI-Detected EMVI and Tumor Deposits and Their Response to Neoadjuvant Therapy in cT3 and cT4 Rectal Cancer . Int J Radiat Oncol Biol Phys 2021. ; 111 ( 3 ): 816 – 825 . - PubMed
-
- Atre ID , Eurboonyanun K , Noda Y , et al . Utility of texture analysis on T2-weighted MR for differentiating tumor deposits from mesorectal nodes in rectal cancer patients, in a retrospective cohort . Abdom Radiol (NY) 2021. ; 46 ( 2 ): 459 – 468 . - PubMed
-
- Altinmakas E , Dogan H , Taskin OC , et al . Extramural venous invasion (EMVI) revisited: a detailed analysis of various characteristics of EMVI and their role as a predictive imaging biomarker in the neoadjuvant treatment response in rectal cancer . Abdom Radiol (NY) 2022. ; 47 ( 6 ): 1975 – 1987 . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
