

Value of a short non-contrast CMR protocol in MINOCA
- PMID: 37581660
- PMCID: PMC10853081
- DOI: 10.1007/s00330-023-10096-2
Value of a short non-contrast CMR protocol in MINOCA
Abstract
Objectives: To evaluate the diagnostic performance of a short non-contrast CMR (ShtCMR) protocol relative to a matched standard comprehensive CMR (StdCMR) protocol in patients with myocardial infarction with non-obstructive coronary arteries (MINOCA).
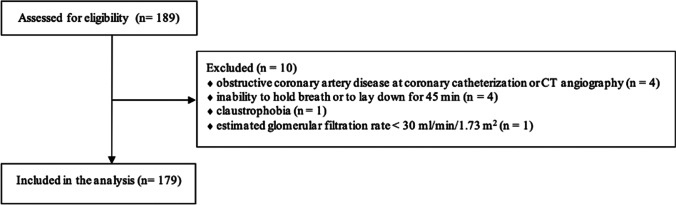
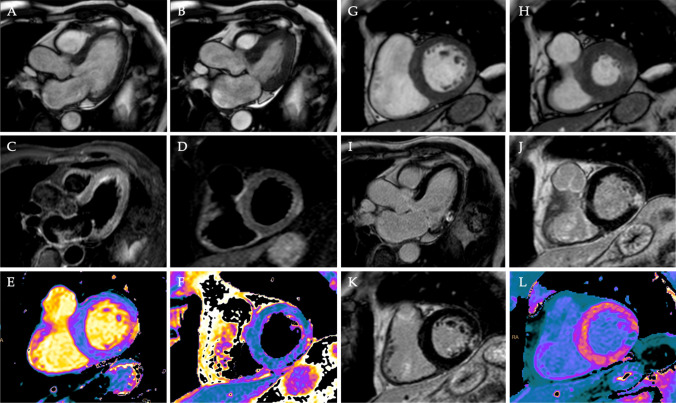
Methods: This multicenter retrospective study included patients with a working diagnosis of MINOCA who underwent a StdCMR between January 2019 and December 2020. An expert and a non-expert reader performed a blinded reading with the ShtCMR (long-axis cine images, T2w-STIR, T1- and T2-mapping). A consensus reading of the StdCMR (reference standard) was performed at least 3 months after the ShtCMR reading session. Readers were asked to report the following: (1) diagnosis; (2) level of confidence in their diagnosis with the ShtCMR; (3) number of myocardial segments involved, and (4) functional parameters.
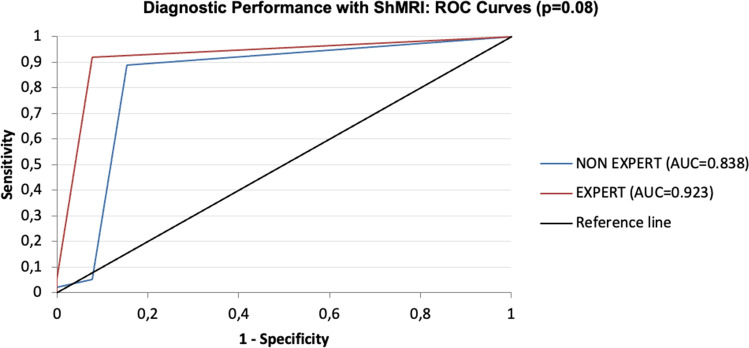
Results: A total of 179 patients were enrolled. The ShtCMR lasted 21 ± 9 min and the StdCMR 45 ± 11 min (p < 0.0001). ShtCMR allowed reaching the same diagnosis as StdCMR in 85% of patients when interpreted by expert readers (rising from 66% for poor confidence to 99% for good, p = 0.0001) and in 73% (p = 0.01) by non-expert ones (60% for poor vs 89% for good confidence, p = 0.0001). Overall, the ShtCMR overestimated the ejection fraction, underestimated cardiac volumes (p < 0.01), and underestimated the number of segments involved by pathology (p = 0.0008) when compared with the StdCMR.
Conclusion: The ShtCMR was found to be a debatable alternative to the StdCMR in patients with MINOCA. Nevertheless, when an experienced reader reaches a good or very good diagnostic confidence using the ShtCMR, the reader may choose to stop the examination, reducing the length of the CMR without affecting the patient's diagnosis.
Clinical relevance statement: A short non-contrast CMR protocol may be a viable alternative to standard protocols in selected CMR studies of patients with MINOCA, allowing for faster diagnosis while reducing time and resources and increasing the number of patients who can be scanned.
Key points: • The ShtCMR lasted 21 ± 9 min and the StdCMR 45 ± 11 min (p < 0.0001). • In 57% of patients with MINOCA, the experienced reader considers that contrast medium is probably not necessary for diagnosis without affecting the patient's diagnosis (99% of agreement rate between ShtCMR and StdCMR).
Keywords: Chest pain; MINOCA; Myocardial infarction; Myocarditis; Takotsubo cardiomyopathy.
© 2023. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures

References
-
- Palmisano A, Vignale D, Tadic M, et al (2022) Myocardial late contrast enhancement CT in troponin-positive acute chest pain syndrome. Radiology 302:545–553 - PubMed
-
- De Ferrari GM, Fox KAA, White JA, et al. Outcomes among non-ST-segment elevation acute coronary syndromes patients with no angiographically obstructive coronary artery disease: observations from 37,101 patients. Eur Heart J Acute Cardiovasc Care. 2014;3:37–45. doi: 10.1177/2048872613489315. - DOI - PMC - PubMed
-
- Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144:e368–e454. - PubMed
