

Manchester Procedure vs Sacrospinous Hysteropexy for Treatment of Uterine Descent: A Randomized Clinical Trial
- PMID: 37581670
- PMCID: PMC10427949
- DOI: 10.1001/jama.2023.13140
Manchester Procedure vs Sacrospinous Hysteropexy for Treatment of Uterine Descent: A Randomized Clinical Trial
Erratum in
-
Addition of Group Name in Byline and Nonauthor Collaborators Supplement.JAMA. 2023 Sep 19;330(11):1101. doi: 10.1001/jama.2023.17655. JAMA. 2023. PMID: 37656447 Free PMC article. No abstract available.
Abstract
Importance: In many countries, sacrospinous hysteropexy is the most commonly practiced uterus-preserving technique in women undergoing a first operation for pelvic organ prolapse. However, there are no direct comparisons of outcomes after sacrospinous hysteropexy vs an older technique, the Manchester procedure.
Objective: To compare success of sacrospinous hysteropexy vs the Manchester procedure for the surgical treatment of uterine descent.
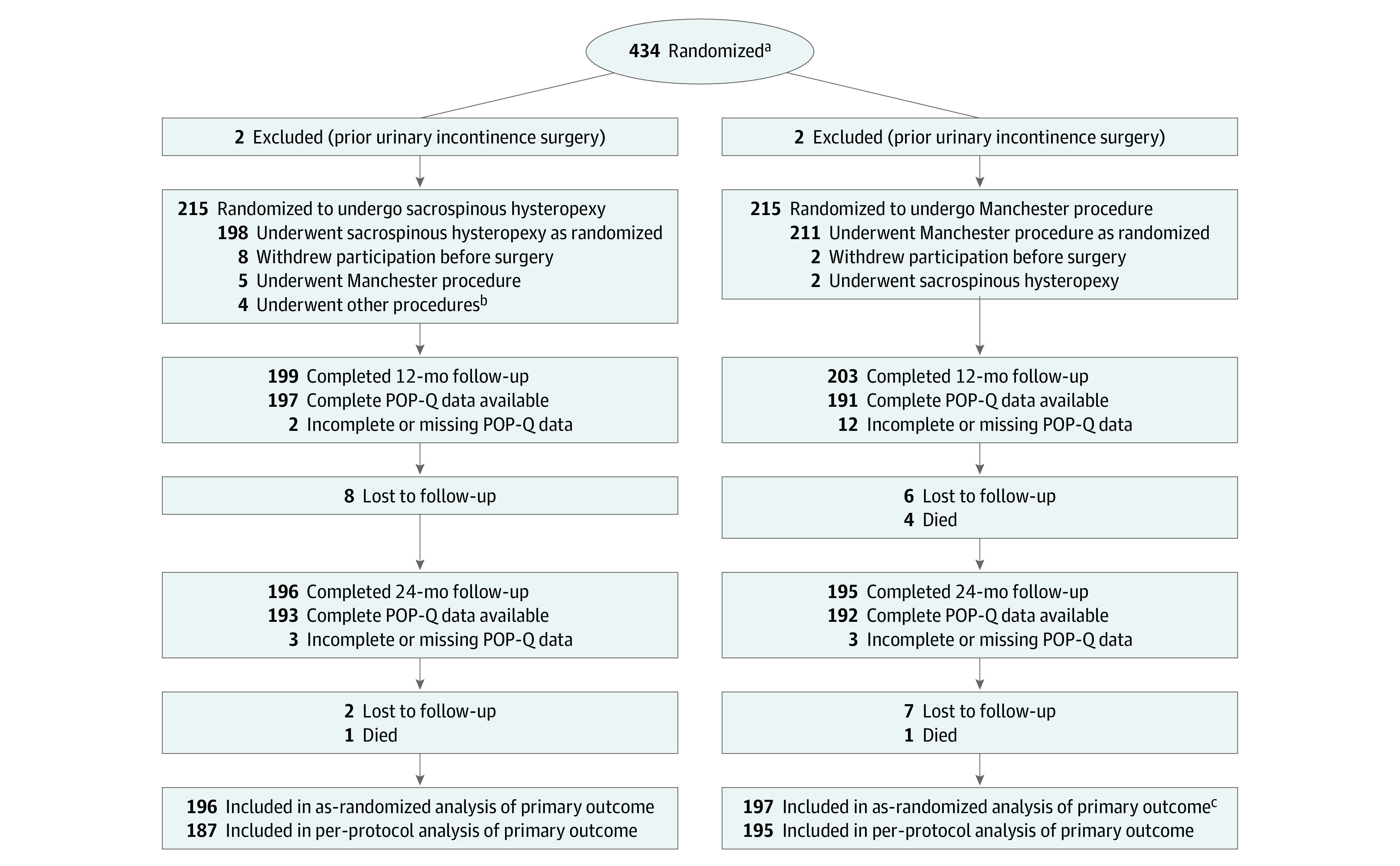
Design, setting, and participants: Multicenter, noninferiority randomized clinical trial conducted in 26 hospitals in the Netherlands among 434 adult patients undergoing a first surgical treatment for uterine descent that did not protrude beyond the hymen.
Interventions: Participants were randomly assigned to undergo sacrospinous hysteropexy (n = 217) or Manchester procedure (n = 217).
Main outcomes and measures: The primary outcome was a composite outcome of success, defined as absence of pelvic organ prolapse beyond the hymen in any compartment evaluated by a standardized vaginal support quantification system, absence of bothersome bulge symptoms, and absence of prolapse retreatment (pessary or surgery) within 2 years after the operation. The predefined noninferiority margin was 9%. Secondary outcomes were anatomical and patient-reported outcomes, perioperative parameters, and surgery-related complications.
Results: Among 393 participants included in the as-randomized analysis (mean age, 61.7 years [SD, 9.1 years]), 151 of 196 (77.0%) in the sacrospinous hysteropexy group and 172 of 197 (87.3%) in the Manchester procedure group achieved the composite outcome of success. Sacrospinous hysteropexy did not meet the noninferiority criterion of -9% for the lower limit of the CI (risk difference, -10.3%; 95% CI, -17.8% to -2.8%; P = .63 for noninferiority). At 2-year follow-up, perioperative outcomes and patient-reported outcomes did not differ between the 2 groups.
Conclusions: Based on the composite outcome of surgical success 2 years after primary uterus-sparing pelvic organ prolapse surgery for uterine descent, these results support a finding that sacrospinous hysteropexy is inferior to the Manchester procedure.
Trial registration: TrialRegister.nl Identifier: NTR 6978.
Conflict of interest statement
Figures

Comment in
-
Updating Evidence for Treatment of Pelvic Organ Prolapse.JAMA. 2023 Aug 15;330(7):599-600. doi: 10.1001/jama.2023.13733. JAMA. 2023. PMID: 37581683 No abstract available.
-
Manchester Procedure vs Sacrospinous Hysteropexy for Pelvic Organ Prolapse.JAMA. 2023 Dec 26;330(24):2394-2395. doi: 10.1001/jama.2023.21795. JAMA. 2023. PMID: 38147099 No abstract available.
References
-
- de Boer TA, Slieker-Ten Hove MC, Burger CW, et al. The prevalence and factors associated with previous surgery for pelvic organ prolapse and/or urinary incontinence in a cross-sectional study in the Netherlands. Eur J Obstet Gynecol Reprod Biol. 2011;158(2):343-349. doi: 10.1016/j.ejogrb.2011.04.029 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
