

Perioperative Vaginal Estrogen as Adjunct to Native Tissue Vaginal Apical Prolapse Repair: A Randomized Clinical Trial
- PMID: 37581673
- PMCID: PMC10427941
- DOI: 10.1001/jama.2023.12317
Perioperative Vaginal Estrogen as Adjunct to Native Tissue Vaginal Apical Prolapse Repair: A Randomized Clinical Trial
Abstract
Importance: Surgical repairs of apical/uterovaginal prolapse are commonly performed using native tissue pelvic ligaments as the point of attachment for the vaginal cuff after a hysterectomy. Clinicians may recommend vaginal estrogen in an effort to reduce prolapse recurrence, but the effects of intravaginal estrogen on surgical prolapse management are uncertain.
Objective: To compare the efficacy of perioperative vaginal estrogen vs placebo cream on prolapse recurrence following native tissue surgical prolapse repair.
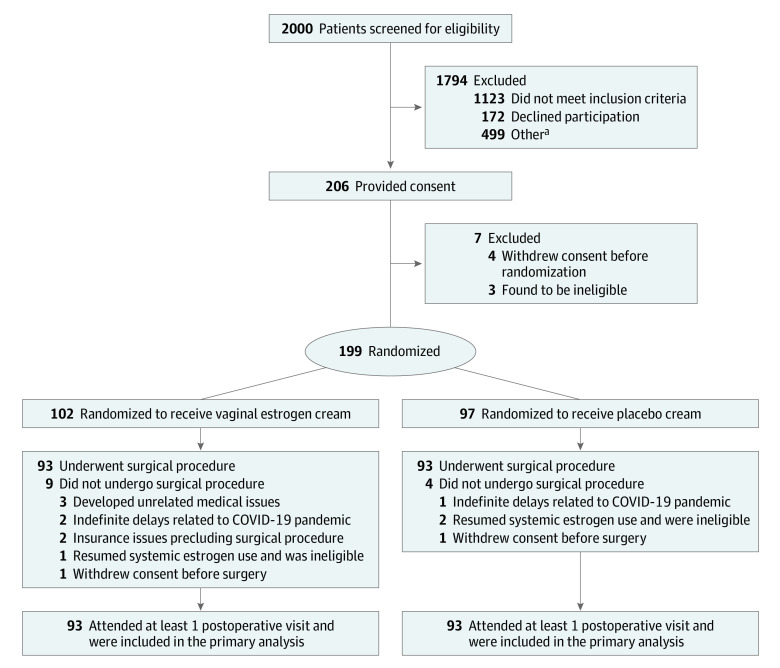
Design, setting, and participants: This randomized superiority clinical trial was conducted at 3 tertiary US clinical sites (Texas, Alabama, Rhode Island). Postmenopausal women (N = 206) with bothersome anterior and apical vaginal prolapse interested in surgical repair were enrolled in urogynecology clinics between December 2016 and February 2020.
Interventions: The intervention was 1 g of conjugated estrogen cream (0.625 mg/g) or placebo, inserted vaginally nightly for 2 weeks and then twice weekly to complete at least 5 weeks of application preoperatively; this continued twice weekly for 12 months postoperatively. Participants underwent a vaginal hysterectomy (if uterus present) and standardized apical fixation (either uterosacral or sacrospinous ligament fixation).
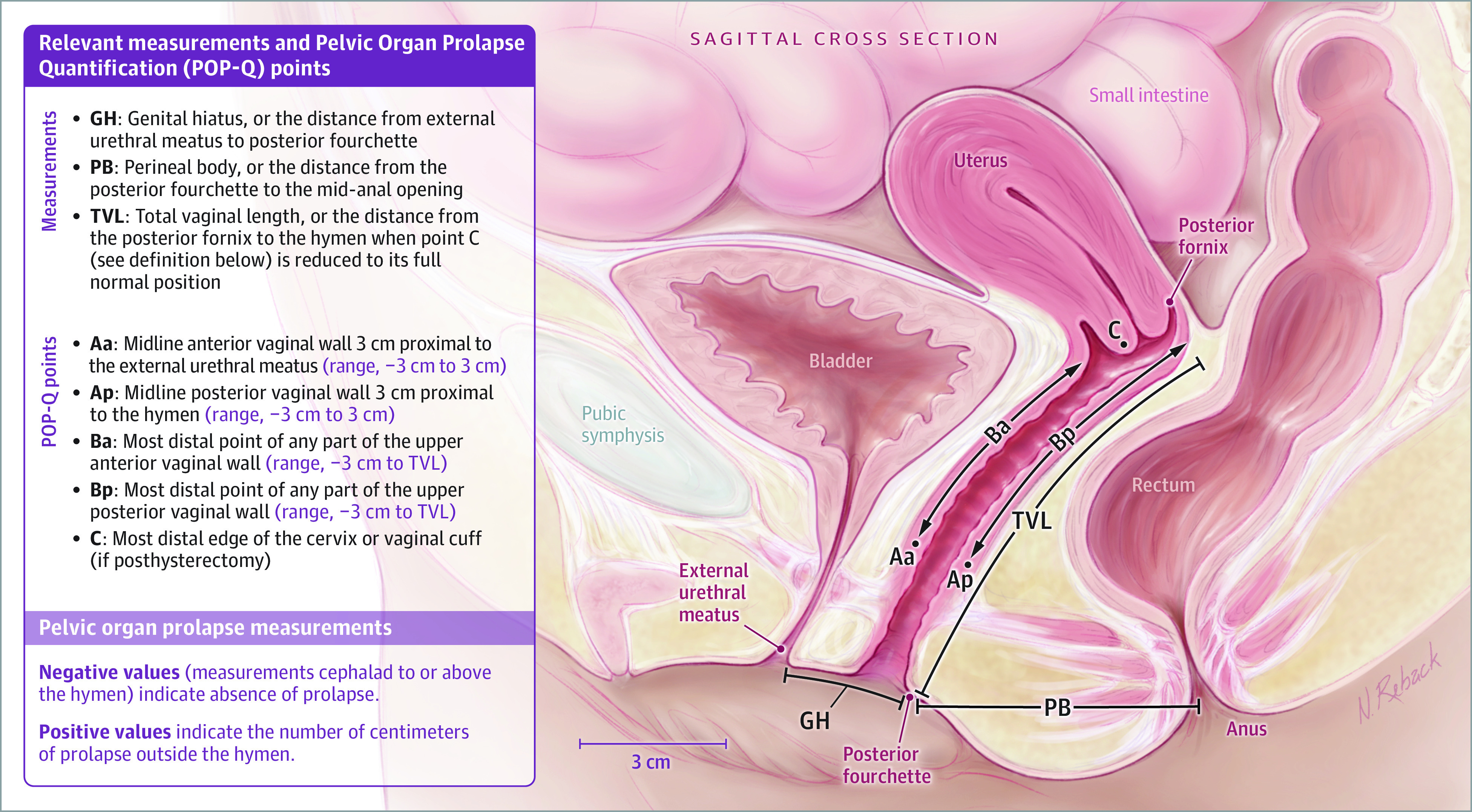
Main outcomes and measures: The primary outcome was time to failure of prolapse repair by 12 months after surgery defined by at least 1 of the following 3 outcomes: anatomical/objective prolapse of the anterior or posterior walls beyond the hymen or the apex descending more than one-third of the vaginal length, subjective vaginal bulge symptoms, or repeated prolapse treatment. Secondary outcomes included measures of urinary and sexual function, symptoms and signs of urogenital atrophy, and adverse events.
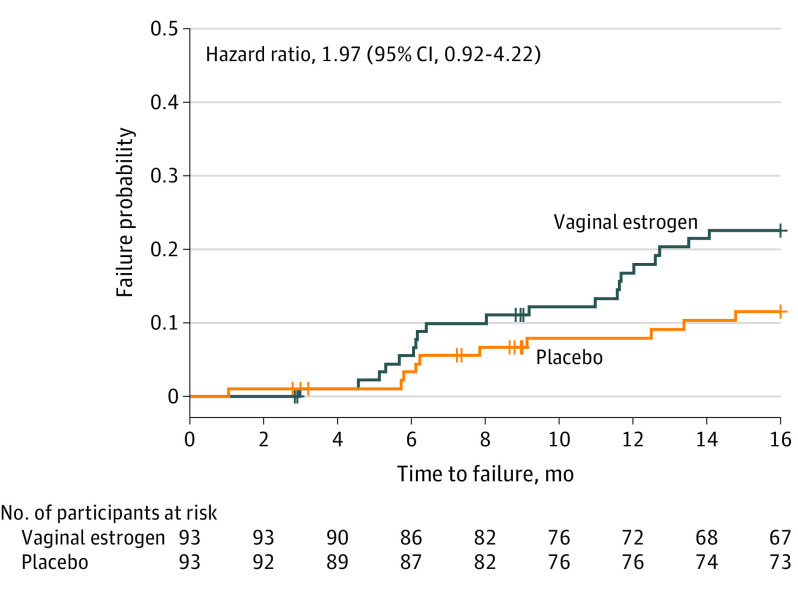
Results: Of 206 postmenopausal women, 199 were randomized and 186 underwent surgery. The mean (SD) age of participants was 65 (6.7) years. The primary outcome was not significantly different for women receiving vaginal estrogen vs placebo through 12 months: 12-month failure incidence of 19% (n = 20) for vaginal estrogen vs 9% (n = 10) for placebo (adjusted hazard ratio, 1.97 [95% CI, 0.92-4.22]), with the anatomic recurrence component being most common, rather than vaginal bulge symptoms or prolapse repeated treatment. Masked surgeon assessment of vaginal tissue quality and estrogenization was significantly better in the vaginal estrogen group at the time of the operation. In the subset of participants with at least moderately bothersome vaginal atrophy symptoms at baseline (n = 109), the vaginal atrophy score for most bothersome symptom was significantly better at 12 months with vaginal estrogen.
Conclusions and relevance: Adjunctive perioperative vaginal estrogen application did not improve surgical success rates after native tissue transvaginal prolapse repair.
Trial registration: ClinicalTrials.gov Identifier: NCT02431897.
Conflict of interest statement
Figures
Comment in
-
Updating Evidence for Treatment of Pelvic Organ Prolapse.JAMA. 2023 Aug 15;330(7):599-600. doi: 10.1001/jama.2023.13733. JAMA. 2023. PMID: 37581683 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
