

Infants Admitted to US Intensive Care Units for RSV Infection During the 2022 Seasonal Peak
- PMID: 37581884
- PMCID: PMC10427947
- DOI: 10.1001/jamanetworkopen.2023.28950
Infants Admitted to US Intensive Care Units for RSV Infection During the 2022 Seasonal Peak
Erratum in
-
Errors in Figure 2, Results, and Tables 1 and 2.JAMA Netw Open. 2024 Jul 1;7(7):e2428669. doi: 10.1001/jamanetworkopen.2024.28669. JAMA Netw Open. 2024. PMID: 39052300 Free PMC article. No abstract available.
Abstract
Importance: Respiratory syncytial virus (RSV) is the leading cause of lower respiratory tract infections (LRTIs) and infant hospitalization worldwide.
Objective: To evaluate the characteristics and outcomes of RSV-related critical illness in US infants during peak 2022 RSV transmission.
Design, setting, and participants: This cross-sectional study used a public health prospective surveillance registry in 39 pediatric hospitals across 27 US states. Participants were infants admitted for 24 or more hours between October 17 and December 16, 2022, to a unit providing intensive care due to laboratory-confirmed RSV infection.
Exposure: Respiratory syncytial virus.
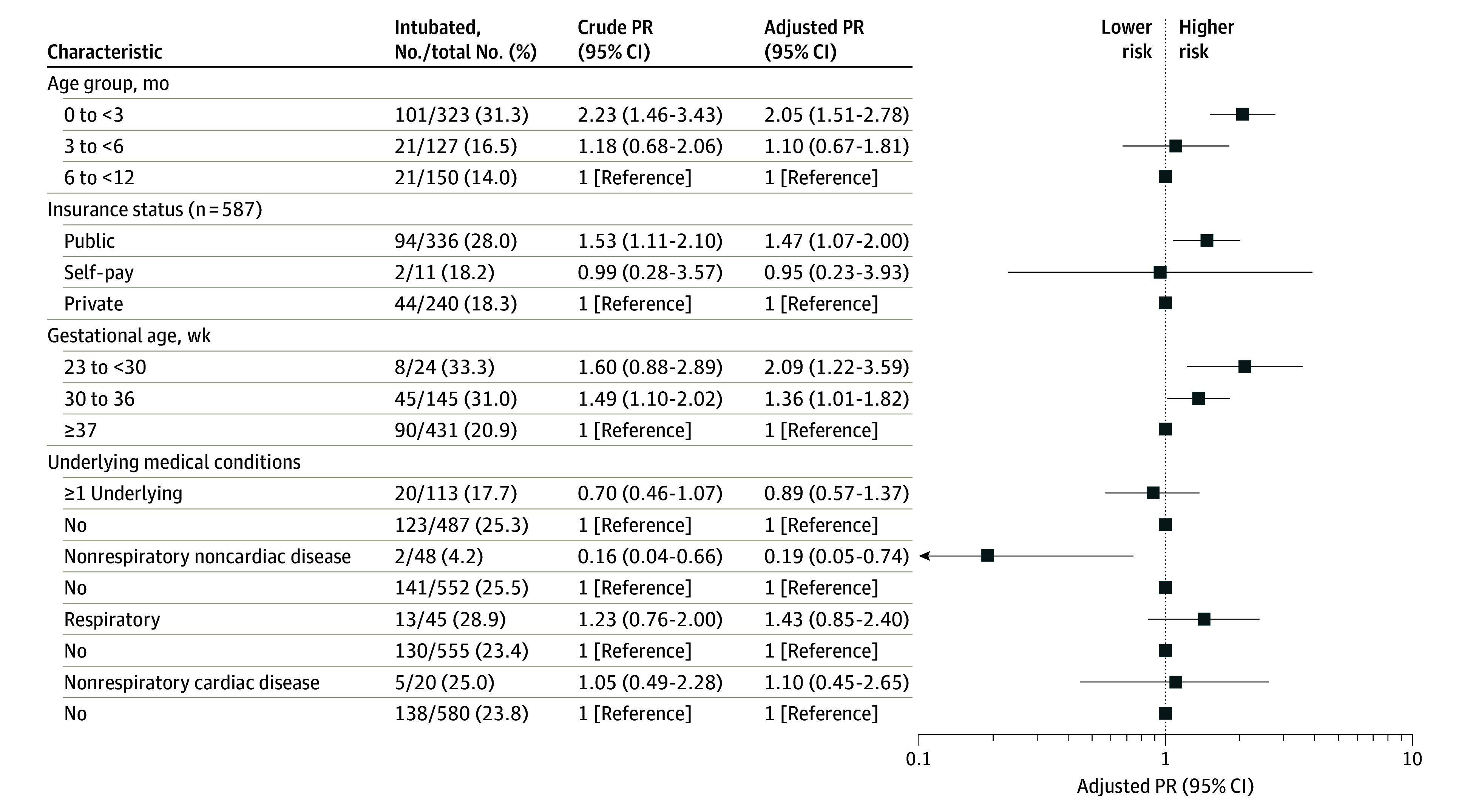
Main outcomes and measures: Data were captured on demographics, clinical characteristics, signs and symptoms, laboratory values, severity measures, and clinical outcomes, including receipt of noninvasive respiratory support, invasive mechanical ventilation, vasopressors or extracorporeal membrane oxygenation, and death. Mixed-effects multivariable log-binomial regression models were used to assess associations between intubation status and demographic factors, gestational age, and underlying conditions, including hospital as a random effect to account for between-site heterogeneity.
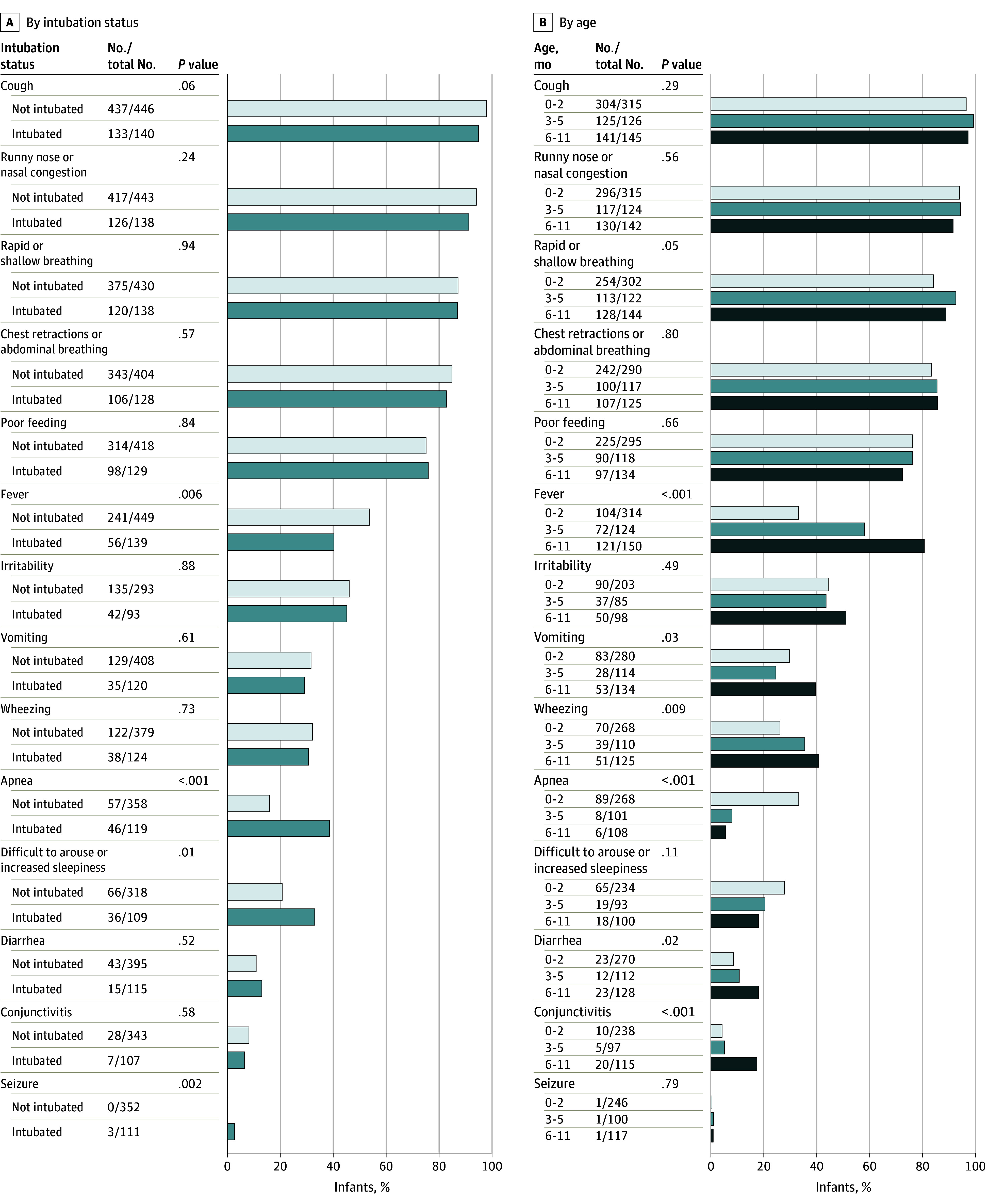
Results: The first 15 to 20 consecutive eligible infants from each site were included for a target sample size of 600. Among the 600 infants, the median (IQR) age was 2.6 (1.4-6.0) months; 361 (60.2%) were male, 169 (28.9%) were born prematurely, and 487 (81.2%) had no underlying medical conditions. Primary reasons for admission included LRTI (594 infants [99.0%]) and apnea or bradycardia (77 infants [12.8%]). Overall, 143 infants (23.8%) received invasive mechanical ventilation (median [IQR], 6.0 [4.0-10.0] days). The highest level of respiratory support for nonintubated infants was high-flow nasal cannula (243 infants [40.5%]), followed by bilevel positive airway pressure (150 infants [25.0%]) and continuous positive airway pressure (52 infants [8.7%]). Infants younger than 3 months, those born prematurely (gestational age <37 weeks), or those publicly insured were at higher risk for intubation. Four infants (0.7%) received extracorporeal membrane oxygenation, and 2 died. The median (IQR) length of hospitalization for survivors was 5 (4-10) days.
Conclusions and relevance: In this cross-sectional study, most US infants who required intensive care for RSV LRTIs were young, healthy, and born at term. These findings highlight the need for RSV preventive interventions targeting all infants to reduce the burden of severe RSV illness.
Conflict of interest statement
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
