

Understanding Perinatal Depression Care Gaps by Examining Care Access and Barriers in Perinatal Individuals With and Without Psychiatric History
- PMID: 37582274
- PMCID: PMC10541927
- DOI: 10.1089/jwh.2022.0306
Understanding Perinatal Depression Care Gaps by Examining Care Access and Barriers in Perinatal Individuals With and Without Psychiatric History
Abstract
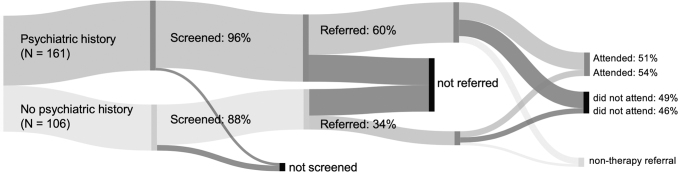
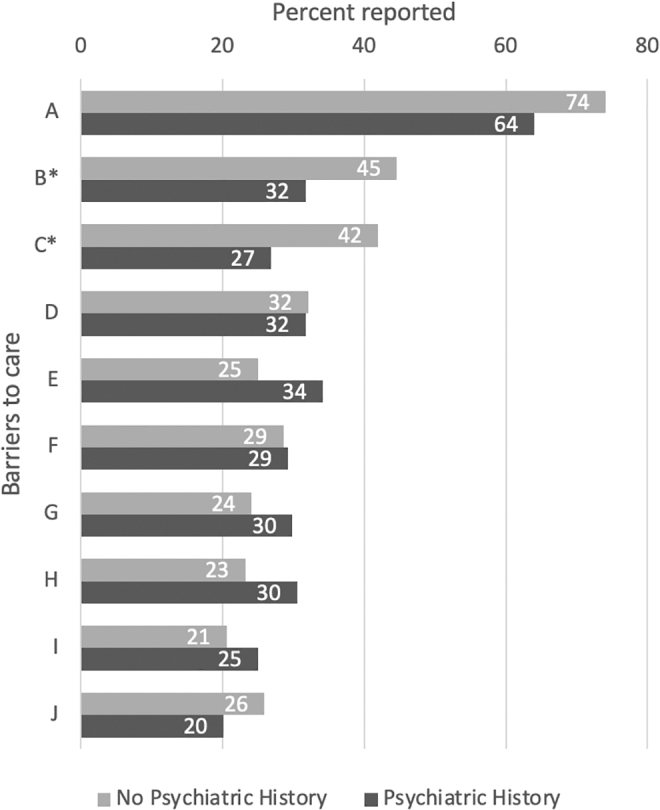
Background: Depression affects one in seven perinatal individuals and remains underdiagnosed and undertreated. Individuals with a psychiatric history are at an even greater risk of perinatal depression, but it is unclear how their experiences with the depression care pathway may differ from individuals without a psychiatric history. Methods: We conducted a secondary analysis evaluating care access and barriers to care in perinatal individuals who screened positive for depression using the Edinburgh Postnatal Depression Scale (N = 280). Data were analyzed from the PRogram in Support of Moms (PRISM) study, a cluster randomized controlled trial of two interventions for perinatal depression. Results: Individuals with no prepregnancy psychiatric history (N = 113), compared with those with a history (N = 167), were less likely to be screened for perinatal depression, and less likely to be offered a therapy referral, although equally likely to attend if referred. When examining how these differences affected outcomes, those without a psychiatric history had 46% lower odds of attending therapy (95% confidence interval [CI]: 0.19-1.55), 79% lower odds of taking medication (95% CI: 0.08-0.54), and 80% lower odds of receiving any depression care (95% CI: 0.08-0.47). Barriers were similar across groups, except for concerns regarding available treatments and beliefs about self-resolution of symptoms, which were more prevalent in individuals without a psychiatric history. Conclusions: Perinatal individuals without a prepregnancy psychiatric history were less likely to be screened, referred, and treated for depression. Differences in screening and referrals resulted in missed opportunities for care, reinforcing the urgent need for universal mental health screening and psychoeducation during the perinatal period. Clinical Trial Registration No.: NCT02935504.
Keywords: barriers; care access; perinatal depression; psychiatric history.
Conflict of interest statement
T.A.M.S. is lead obstetric engagement liaison as a consultant for the MCPAP for Moms and as such has received a stipend from the Massachusetts Department of Mental Health
N.B. has received salary and/or funding support from Massachusetts Department of Mental Health
Figures
References
-
- Stark E, Shim J, Ross C, et al. The impact of perinatal depression on breastfeeding rates. Obstet Gynecol 2018;131(1):122S–123S; doi: 10.1097/01.aog.0000533518.70477.73 - DOI
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
