

Visual System Involvement in Glial Fibrillary Acidic Protein Astrocytopathy: Two Case Reports and a Systematic Literature Review
- PMID: 37582612
- PMCID: PMC10427126
- DOI: 10.1212/NXI.0000000000200146
Visual System Involvement in Glial Fibrillary Acidic Protein Astrocytopathy: Two Case Reports and a Systematic Literature Review
Erratum in
-
Missing Full Disclosures.Neurol Neuroimmunol Neuroinflamm. 2025 Jan;12(1):e200342. doi: 10.1212/NXI.0000000000200342. Epub 2024 Oct 30. Neurol Neuroimmunol Neuroinflamm. 2025. PMID: 39475708 Free PMC article. No abstract available.
Abstract
Background and objectives: Glial fibrillary acidic protein (GFAP) antibodies can associate with an astrocytopathy often presenting as a meningoencephalitis. Visual involvement has been reported but scarcely defined. We describe 2 cases of GFAP astrocytopathy with predominant visual symptoms and present a systematic review of the literature.
Methods: We describe 2 patients with GFAP astrocytopathy from our neurology department. We performed a systematic review of the literature according to PRISMA guidelines, including all patients with this disease and available clinical data, focusing on visual involvement.
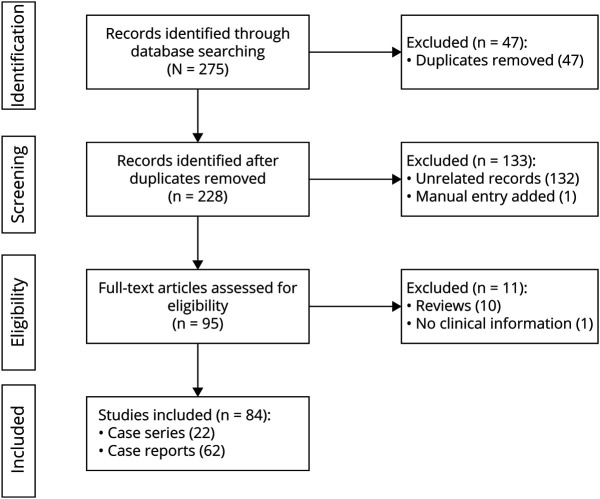
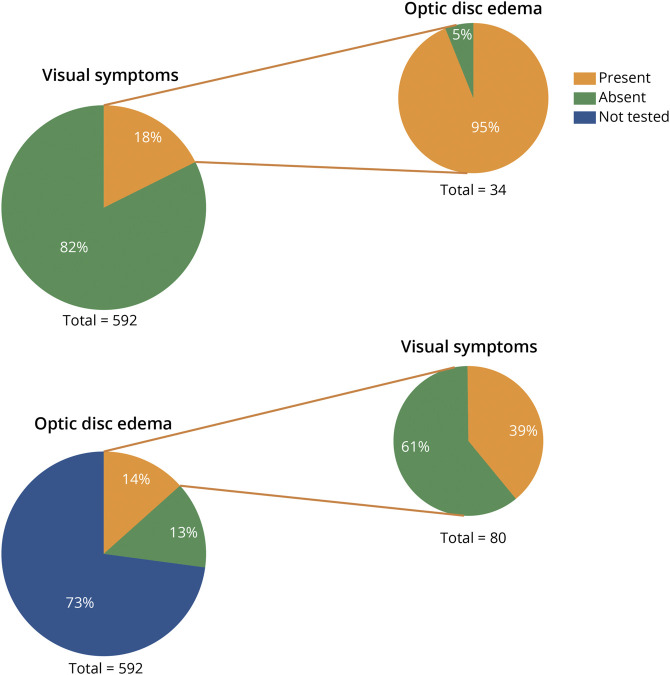
Results: Patient 1 presented with bilateral optic disc edema and severe sudden bilateral loss of vision poorly responsive to therapy. Patient 2 showed bilateral optic disc edema, headache, and mild visual loss with complete recovery after steroids. We screened 275 records and included 84 articles (62 case reports and 22 case series) for a total of 592 patients. Visual involvement was reported in 149/592 (25%), with either clinical symptoms or paraclinical test-restricted abnormalities. Bilateral optic disc edema was found in 80/159 (50%) of patients investigated with fundoscopy, among which 49/80 (61%) were asymptomatic. One hundred (100/592, 17%) reported visual symptoms, often described as blurred vision or transient visual obscurations. Optic neuritis was rare and diagnosed in only 6% of all patients with GFAP astrocytopathy, often without consistent clinical and paraclinical evidence to support the diagnosis. Four patients (including patient 1) manifested a severe, bilateral optic neuritis with poor treatment response. In patients with follow-up information, a relapsing disease course was more frequently observed in those with vs without visual involvement (35% vs 11%, p = 0.0035, OR 3.6 [CI 1.44-8.88]).
Discussion: Visual system involvement in GFAP astrocytopathy is common and heterogeneous, ranging from asymptomatic bilateral optic disc edema to severe bilateral loss of vision, but optic neuritis is rare. GFAP CSF antibody testing should be considered in patients with encephalitis/meningoencephalitis or myelitis and bilateral optic disc edema, even without visual symptoms, and in patients with severe bilateral optic neuritis, especially when AQP4 antibodies are negative. Visual symptoms might associate with a higher relapse risk and help to identify patients who may require chronic immunosuppression.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous