

Mimics of Autoimmune Encephalitis: Validation of the 2016 Clinical Autoimmune Encephalitis Criteria
- PMID: 37582614
- PMCID: PMC10427145
- DOI: 10.1212/NXI.0000000000200148
Mimics of Autoimmune Encephalitis: Validation of the 2016 Clinical Autoimmune Encephalitis Criteria
Erratum in
-
Missing Full Disclosures.Neurol Neuroimmunol Neuroinflamm. 2025 Jan;12(1):e200342. doi: 10.1212/NXI.0000000000200342. Epub 2024 Oct 30. Neurol Neuroimmunol Neuroinflamm. 2025. PMID: 39475708 Free PMC article. No abstract available.
Abstract
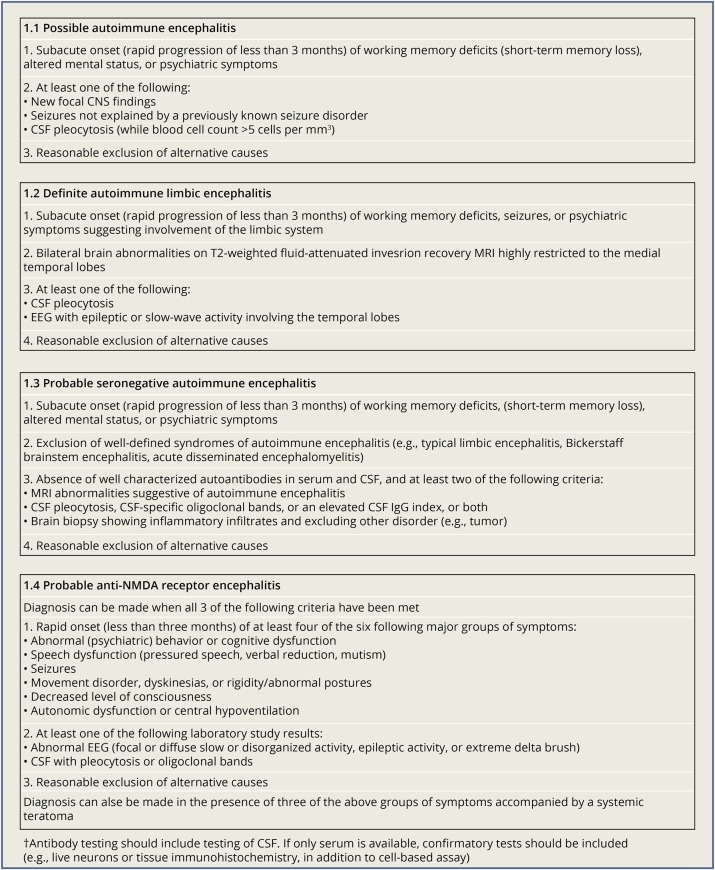
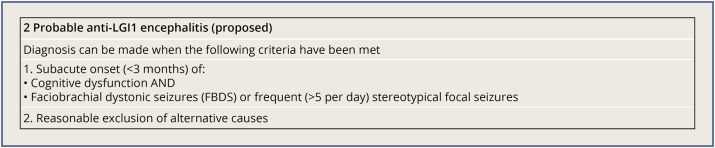
Background and objectives: The clinical criteria for autoimmune encephalitis (AE) were proposed by Graus et al. in 2016. In this study, the AE criteria were validated in the real world, and common AE mimics were described. In addition, criteria for probable anti-LGI1 encephalitis were proposed and validated.
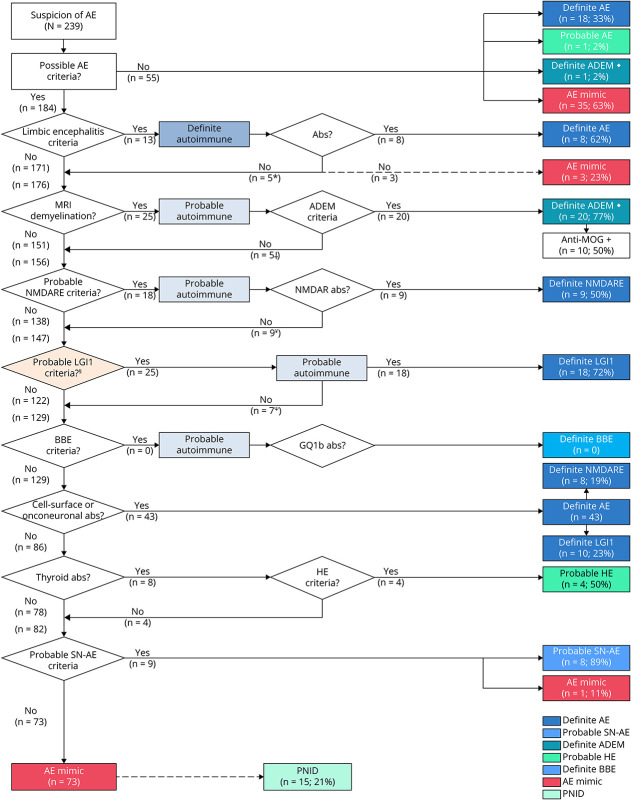
Methods: In this retrospective cohort study, patients referred to our national referral center with suspicion of AE and specific neuroinflammatory disorders with similar clinical presentations were included from July 2016 to December 2019. Exclusion criteria were pure cerebellar or peripheral nerve system disorders. All patients were evaluated according to the AE criteria.
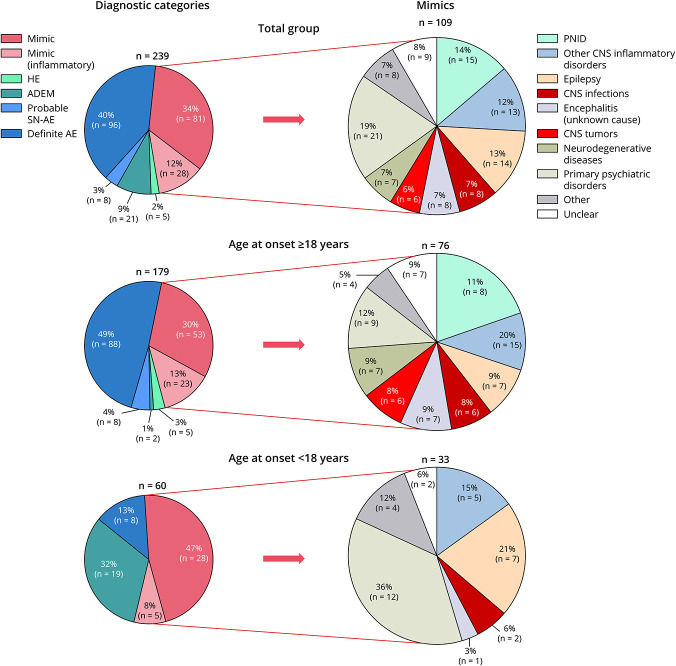
Results: In total, 239 patients were included (56% female; median age 42 years, range 1-85). AE was diagnosed in 104 patients (44%) and AE mimics in 109 patients (46%). The most common AE mimics and misdiagnoses were neuroinflammatory CNS disorders (26%), psychiatric disorders (19%), epilepsy with a noninflammatory cause (13%), CNS infections (7%), neurodegenerative diseases (7%), and CNS neoplasms (6%). Common confounding factors were mesiotemporal lesions on brain MRI (17%) and false-positive antibodies in serum (12%). Additional mesiotemporal features (involvement extralimbic structures, enhancement, diffusion restriction) were observed more frequently in AE mimics compared with AE (61% vs 24%; p = 0.005). AE criteria showed the following sensitivity and specificity: possible AE, 83% (95% CI 74-89) and 27% (95% CI 20-36); definite autoimmune limbic encephalitis (LE), 10% (95% CI 5-17) and 98% (95% CI 94-100); and probable anti-NMDAR encephalitis, 50% (95% CI 26-74) and 96% (95% CI 92-98), respectively. Specificity of the criteria for probable seronegative AE was 99% (95% CI 96-100). The newly proposed criteria for probable anti-LGI1 encephalitis showed a sensitivity of 66% (95% CI 47-81) and specificity of 96% (95% CI 93-98).
Discussion: AE mimics occur frequently. Common pitfalls in AE misdiagnosis are mesiotemporal lesions (predominantly with atypical features) and false-positive serum antibodies. As expected, the specificity of the criteria for possible AE is low because these criteria represent the minimal requirements for entry in the diagnostic algorithm for AE. Criteria for probable AE (-LGI1, -NMDAR, seronegative) and definite autoimmune LE are applicable for decisions on immunotherapy in early disease stage, as specificity is high.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Conflict of interest statement
P.A. Sillevis Smitt holds a patent for the detection of anti-DNER, he received research support from Euroimmun. R.F. Neuteboom reports participates in pediatric MS studies with Novartis, Roche, and Sanofi-Genzyme; he received consultancy fees from Novartis, Sanofi-Genzyme, and Zogenix; he received research grants from the Dutch MS research foundation, DreaMS foundation, Postcode Loterij, Vrienden Loterij, Stichting Vrienden van het Sophia. M.J. Titulaer has filed a patent, on behalf of the Erasmus MC, for methods for typing neurologic disorders and cancer, and devices for use therein; has received research funds for serving on a scientific advisory board of Horizon Therapeutics, for consultation at Guidepoint Global LLC, for consultation at UCB, for teaching colleagues at Novartis; and has received an unrestricted research grant from Euroimmun AG and from CSL Behring. The other authors report no relevant disclosures. Go to
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Research Materials