

LGI1 Encephalitis and IgG4-Related Disease: Rare Conditions Collide
- PMID: 37582616
- PMCID: PMC10427142
- DOI: 10.1212/NXI.0000000000200158
LGI1 Encephalitis and IgG4-Related Disease: Rare Conditions Collide
Erratum in
-
Missing Full Disclosures.Neurol Neuroimmunol Neuroinflamm. 2025 Jan;12(1):e200342. doi: 10.1212/NXI.0000000000200342. Epub 2024 Oct 30. Neurol Neuroimmunol Neuroinflamm. 2025. PMID: 39475708 Free PMC article. No abstract available.
Abstract
Objectives: Leucine-rich glioma-inactivated 1 (LGI1) encephalitis and IgG4-related disease (IgG4RD) have traditionally been regarded as 2 distinct disease entities.
Methods: We detail the presentation, investigations, and management of a patient who showed typical signs and symptoms of LGI1 encephalitis and also found to possess pancreatic changes and a serum profile in keeping with IgG4RD.
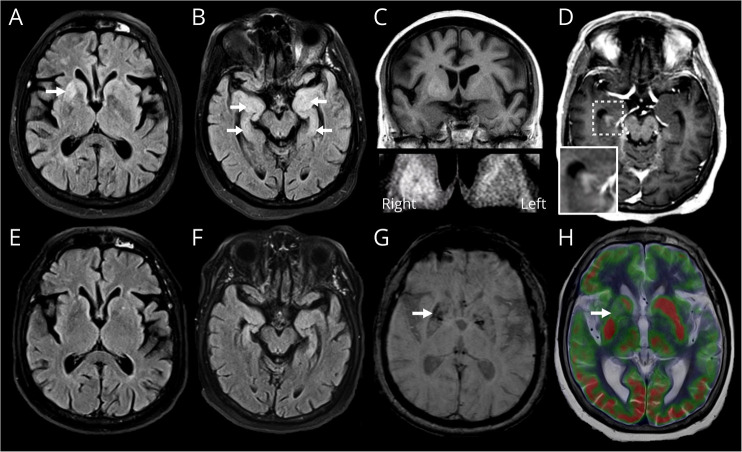
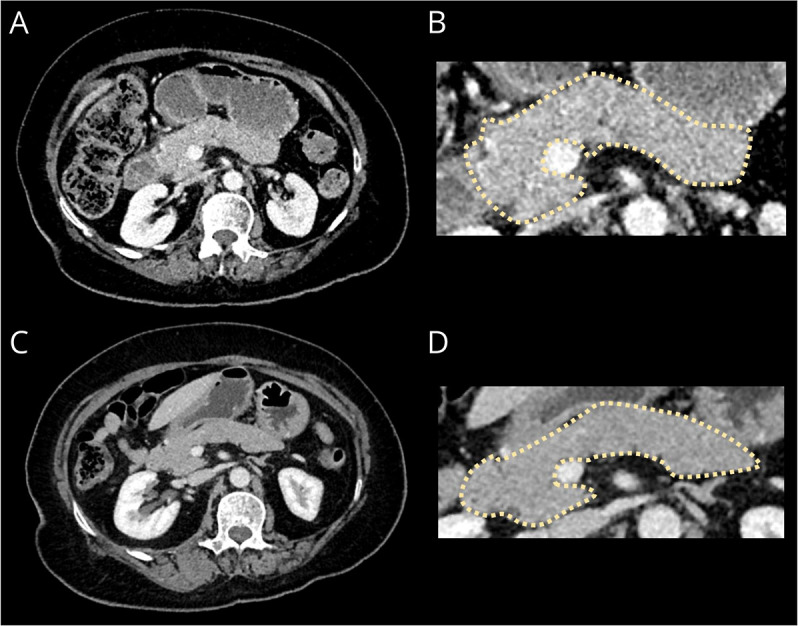
Results: Serum and CSF analyses at presentation showed a significant hyponatraemia (117 mmol/L), elevated IgG4 concentration (1.73 g/L), and the presence of LGI1 antibodies. MRI revealed symmetrical diffuse T2-weighted hyperintensity and mild swelling throughout both medial temporal lobes. CT of the chest, abdomen and pelvis revealed an edematous, bulky pancreas with loss of lobulation, typical for IgG4RD. A glucocorticoid weaning regimen was commenced, facilitated by 2 rituximab infusions, with the patient showing an effective treatment response. HLA testing confirmed the presence of HLA DRB1 and HLA DQB1 risk alleles.
Discussion: This case suggests that there may be shared mechanisms between LGI1 encephalitis and IgG4RD, supported by common risk HLA associations and treatment strategies/responses. To our knowledge, this represents the first instance that LGI1 encephalitis and IgG4RD have been reported in the same patient and emphasizes the continued development of our understanding of the wide range of IgG4-mediated conditions.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures
References
-
- Culver EL, Sadler R, Simpson D, et al. . Elevated serum IgG4 levels in diagnosis, treatment response, organ involvement, and relapse in a prospective IgG4-related disease UK cohort. Am J Gastroenterol. 2016;111(5):733-743. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials