

Renal tubular acidosis without interstitial nephritis in Sjögren's syndrome: a case report and review of the literature
- PMID: 37582721
- PMCID: PMC10426178
- DOI: 10.1186/s12882-023-03290-3
Renal tubular acidosis without interstitial nephritis in Sjögren's syndrome: a case report and review of the literature
Abstract
Background: Renal tubular acidosis is the principal clinical feature associated with tubulointerstitial nephritis in patients with primary Sjögren's syndrome. Renal tubular dysfunction due to interstitial nephritis has been considered the underlying pathophysiology connecting renal tubular acidosis and primary Sjögren's syndrome. However, the detailed mechanisms underlying the pathophysiology of renal tubular acidosis in primary Sjögren's syndrome is not fully understood.
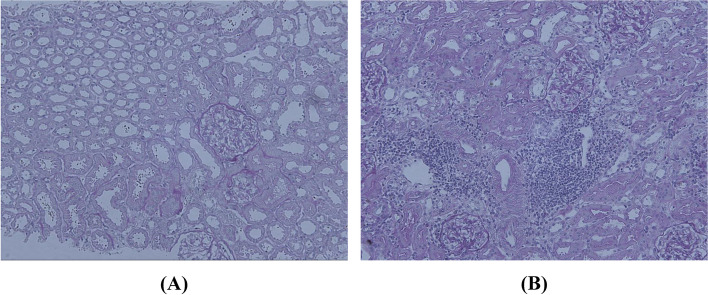
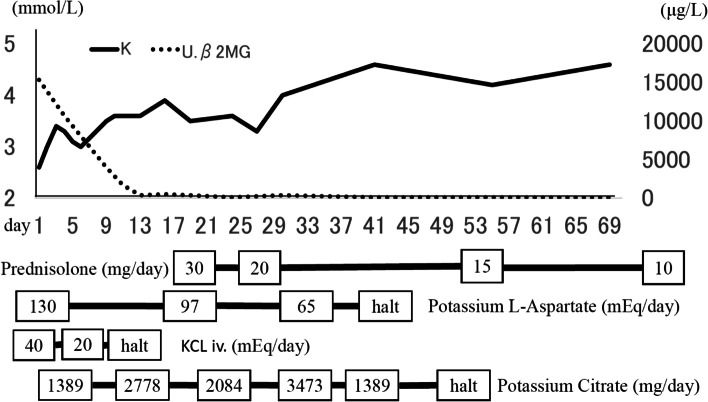
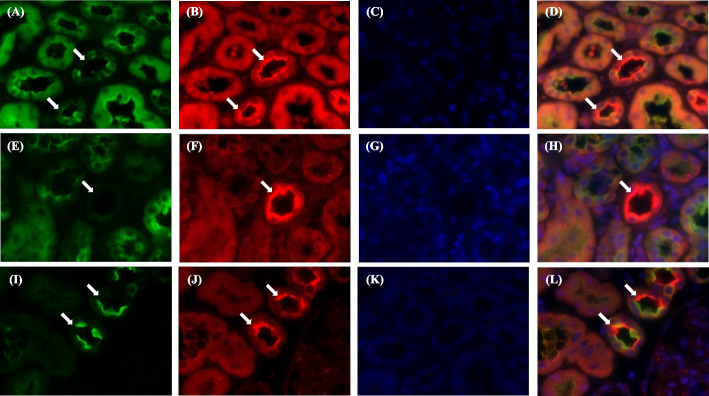
Case presentation: A 30-year-old woman was admitted with complaints of weakness in the extremities. The patient was hospitalized thirteen years earlier for similar issues and was diagnosed with hypokalemic paralysis due to distal renal tubular acidosis with primary Sjögren's syndrome. This diagnosis was based on a positive Schirmer's test. Besides, anti-Sjögren's syndrome-related antigen A was also detected. Laboratory tests indicated distal RTA; however, a renal biopsy showed no obvious interstitial nephritis. Laboratory tests conducted during the second admission indicated distal renal tubular acidosis. Therefore, a renal biopsy was performed again, which revealed interstitial nephritis. Histological analysis of acid-base transporters revealed the absence of vacuolar type H+-ATPases in the collecting duct. The vacuolar type H+-ATPase was also absent in the past renal biopsy, suggesting that the alteration in acid-base transporters is independent of interstitial nephritis.
Conclusions: This case study demonstrates that vacuolar-type H+-ATPases are associated with distal renal tubular acidosis, and distal renal tubular acidosis precedes interstitial nephritis in patients with primary Sjögren's syndrome.
Keywords: H+-ATPase; Hypokalemia; Interstitial nephritis; Renal tubular acidosis; SJÖGREN’S syndrome.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Coexistence of Sjögren's Syndrome-associated Interstitial Nephritis and Hypokalemic Nephropathy in a Patient with Distal Renal Tubular Acidosis.Intern Med. 2025 Apr 1;64(7):1067-1074. doi: 10.2169/internalmedicine.4152-24. Epub 2024 Aug 28. Intern Med. 2025. PMID: 39198164 Free PMC article.
-
An unusual case of hypokalemic paralysis associated with primary Sjogren's syndrome.J Ark Med Soc. 2008 Jun;104(12):286-7. J Ark Med Soc. 2008. PMID: 18564466
-
Hypokalemic paralysis and osteomalacia secondary to renal tubular acidosis in a case with primary Sjögren's syndrome.Mod Rheumatol. 2006;16(1):48-51. doi: 10.1007/s10165-005-0446-2. Mod Rheumatol. 2006. PMID: 16622725
-
Fanconi's syndrome and distal (type 1) renal tubular acidosis in a patient with primary Sjögren's syndrome with monoclonal gammopathy of undetermined significance.Clin Nephrol. 2006 Jun;65(6):427-32. doi: 10.5414/cnp65427. Clin Nephrol. 2006. PMID: 16792139 Review.
-
Tubulointerstitial nephritis and Fanconi syndrome in a patient with primary Sjögren's syndrome accompanied by antimitochondrial antibodies: A case report and review of the literature.Mod Rheumatol. 2018 Sep;28(5):897-900. doi: 10.3109/14397595.2016.1174422. Epub 2016 May 4. Mod Rheumatol. 2018. PMID: 27142563 Review.
Cited by
-
Coexistence of Sjögren's Syndrome-associated Interstitial Nephritis and Hypokalemic Nephropathy in a Patient with Distal Renal Tubular Acidosis.Intern Med. 2025 Apr 1;64(7):1067-1074. doi: 10.2169/internalmedicine.4152-24. Epub 2024 Aug 28. Intern Med. 2025. PMID: 39198164 Free PMC article.
-
Sjogren's Syndrome Presenting With Proximal Myopathy Due to Osteomalacia Complicating Renal Tubular Acidosis: A Case Report.Cureus. 2025 Apr 13;17(4):e82206. doi: 10.7759/cureus.82206. eCollection 2025 Apr. Cureus. 2025. PMID: 40370894 Free PMC article.
-
A case of Sjögren's syndrome with selective anion exchanger 1 defect causing distal renal tubular acidosis.Pediatr Nephrol. 2025 Jun;40(6):1899-1902. doi: 10.1007/s00467-024-06641-w. Epub 2025 Jan 13. Pediatr Nephrol. 2025. PMID: 39804391
References
-
- Ramos-Casals M, Brito-Zerón P, Seror R, Bootsma H, Bowman SJ, Dörner T, et al. Characterization of systemic disease in primary sjögren’s syndrome: EULAR-SS task force recommendations for articular, cutaneous, pulmonary, and renal involvements. Rheumatol (Oxford) 2015;54:2230–2238. doi: 10.1093/rheumatology/kev200. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
