

Contributing factors of birth asphyxia in Thailand: a case-control study
- PMID: 37582743
- PMCID: PMC10426058
- DOI: 10.1186/s12884-023-05885-y
Contributing factors of birth asphyxia in Thailand: a case-control study
Abstract
Background: Birth asphyxia is of significant concern because it impacts newborn health from low to severe levels. In Thailand, birth asphyxia remains a leading cause of delayed developmental health in children under 5 years old. The study aimed to determine the maternal, fetal and health service factors contributing to birth asphyxia.
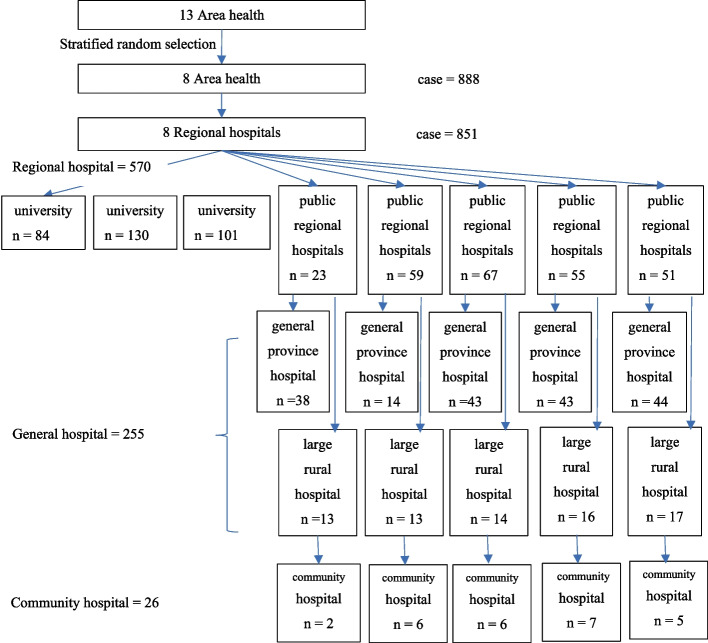
Methods: A case-control design was conducted on a sample of 4256 intrapartum chart records. The samples were selected based on their Apgar scores in the first minute of life. A low Apgar score (≤ 7) was chosen for the case group (852) and a high Apgar score (> 7) for the control group (3408). In addition, a systematic random technique was performed to select 23 hospitals, including university, advanced and secondary, in eight health administration areas in Thailand for evaluating the intrapartum care service. Data analysis was conducted using SPSS statistical software.
Results: The odds of birth asphyxia increases in the university and advanced hospitals but the university hospitals had the highest quality of care. The advanced and secondary hospitals had average nurse work-hours per week of more than 40 h. Multivariable logistic regression analysis found that intrapartum care services and maternal-fetal factors contributed to birth asphyxia. The odd of birth asphyxia increases significantly in late-preterm, late-term pregnancies, low-birth weight, and macrosomia. Furthermore, maternal comorbidity, non-reassuring, and obstetric emergency conditions significantly increase the odd of birth asphyxia. In addition, an excellent quality of intrapartum care, a combined nursing model, low nurse work-hours, and obstetrician-conducted delivery significantly reduced birth asphyxia.
Conclusion: Birth asphyxia problems may be resolved in the health service management offered by reducing the nurse work-hours. Excellent quality of care required the primary nursing care model combined with a team nursing care model. However, careful evaluation and monitoring are needed in cases of comorbidity, late-preterm, late-term pregnancies, low-birth weight, and macrosomia. Furthermore, increasing the obstetrician availability in obstetric emergencies and non-reassuring fetal status is important.
Keywords: Birth asphyxia; Intrapartum care service; Quality of care.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
Ethical approval for the study was obtained from the Siriraj Institutional Review Board of the Faculty of Medicine, Mahidol University (No. Si 705/2018); the Human Research Ethics Committee, Faculty of Medicine, Prince of Songkla University (REC. 61–317-19–6); and the Research Ethics Committee, Faculty of Medicine, Chiang Mai University (ID: 5649). The ethics committee complies fully with international guidelines for human research protection, such as the Declaration of Helsinki, the Belmont Report, CIOMS Guidelines and the International Conference on Harmonization in Good Clinical Practice (ICH-GCP). The research proposal, participant information sheet, informed consent form, case record form and questionnaire were approved. Before data collection, human research protection certificates were presented to each hospital director of the research setting for permission. All agreed to permit data collection before the data collection began. All the enrolled head nurses of the intrapartum unit were accurately informed about the research purpose, and the researcher randomly selected the samples based on the inclusion criteria.
The data collection progress must be reported at least once a year except where required more frequent by the Research Ethics Committee. Prior Research Ethics Committee approval is required before implementing any changes in the consent documents or protocol unless those changes are needed urgently for the safety of subjects. In addition, any event or new information that may affect the benefit/risk ratio of the study must be reported to the research ethic committee promptly.
The informed consent was performed in a voluntary approached before data collection from the participant. Each participant was adequately informed of the aims, methods, possible conflicts of interest, institutional affiliations of the researcher, the anticipated benefits and potential risks of the study and the discomfort it may entail, post-study provisions and any other relevant aspects of the study. In addition, the participant was informed about the right to withdraw consent to participate at any time without reprisal.
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
