

The potential link between acromegaly and risk of acute ischemic stroke in patients with pituitary adenoma: a new perspective
- PMID: 37584889
- PMCID: PMC11139727
- DOI: 10.1007/s13760-023-02354-3
The potential link between acromegaly and risk of acute ischemic stroke in patients with pituitary adenoma: a new perspective
Abstract
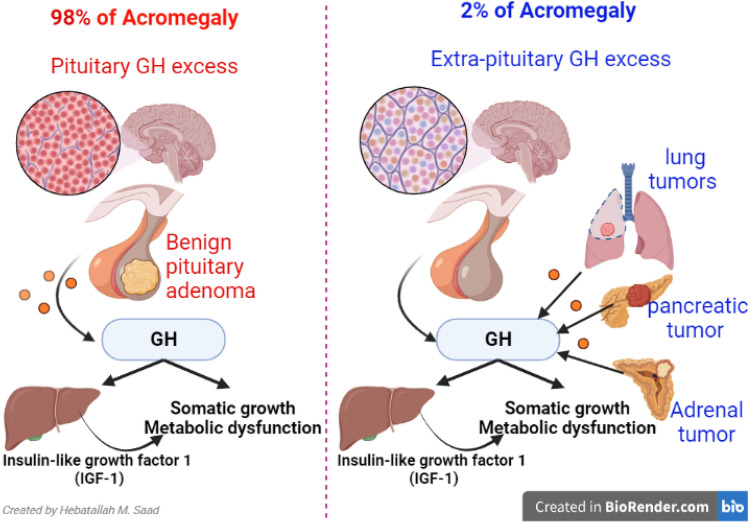
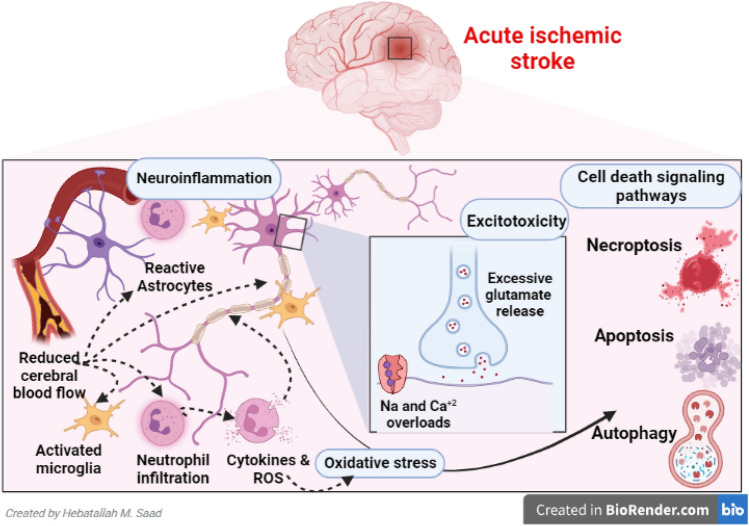
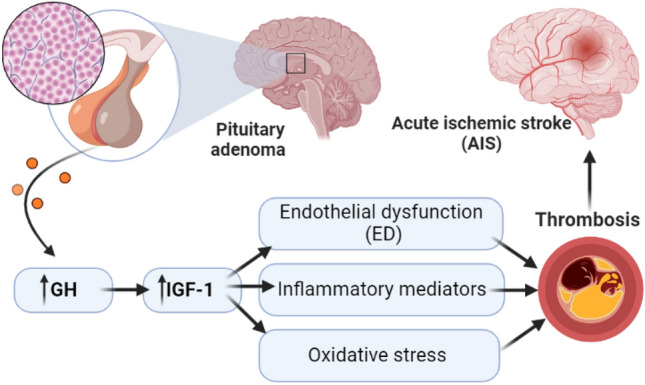
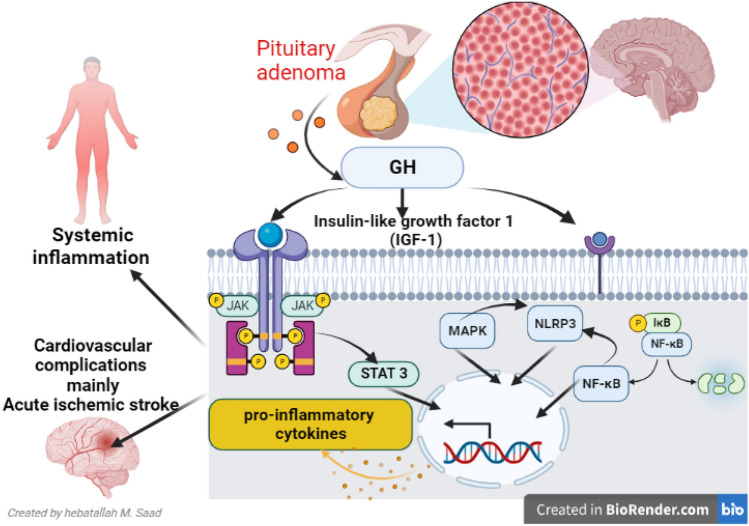
Acromegaly is an endocrine disorder due to the excess production of growth hormone (GH) from the anterior pituitary gland after closed epiphyseal growth plates. Acromegaly is mainly caused by benign GH-secreting pituitary adenoma. Acute ischemic stroke (AIS) is one of the most common cardiovascular complications. It ranks second after ischemic heart disease (IHD) as a cause of disability and death in high-income countries globally. Thus, this review aimed to elucidate the possible link between acromegaly and the development of AIS. The local effects of acromegaly in the development of AIS are related to the development of pituitary adenoma and associated surgical and radiotherapies. Pituitary adenoma triggers the development of AIS through different mechanisms, particularly aneurysmal formation, associated thrombosis, and alteration of cerebral microcirculation. Cardiovascular complications and mortality were higher in patients with pituitary adenoma. The systemic effect of acromegaly-induced cardio-metabolic disorders may increase the risk for the development of AIS. Additionally, acromegaly contributes to the development of endothelial dysfunction (ED), inflammatory and oxidative stress, and induction of thrombosis that increases the risk for the development of AIS. Moreover, activated signaling pathways, including activator of transcription 3 (STAT3), nuclear factor kappa B (NF-κB), nod-like receptor pyrin 3 (NLRP3) inflammasome, and mitogen-activated protein kinase (MAPK) in acromegaly may induce systemic inflammation with the development of cardiovascular complications mainly AIS. Taken together, acromegaly triggers the development of AIS through local and systemic effects by inducing the formation of a cerebral vessel aneurysm, the release of pro-inflammatory cytokines, the development of oxidative stress, ED, and thrombosis correspondingly.
Keywords: Acromegaly; Acute ischemic stroke; Growth hormone; Insulin-like growth factor 1.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
