

Bioengineered human tissue regeneration and repair using endogenous stem cells
- PMID: 37586324
- PMCID: PMC10439273
- DOI: 10.1016/j.xcrm.2023.101156
Bioengineered human tissue regeneration and repair using endogenous stem cells
Abstract
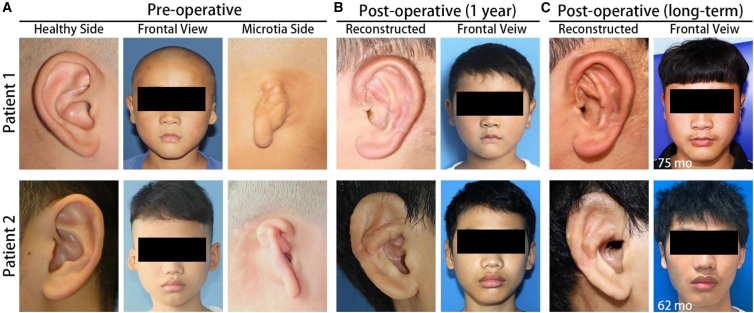
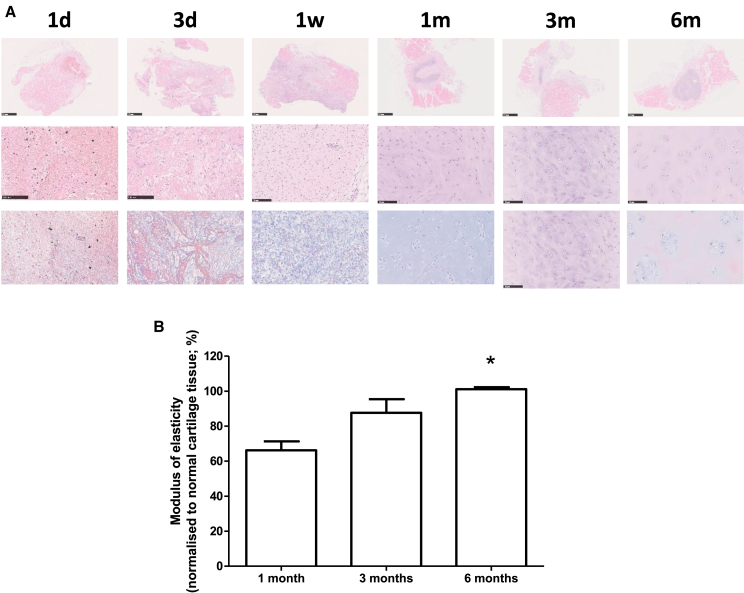
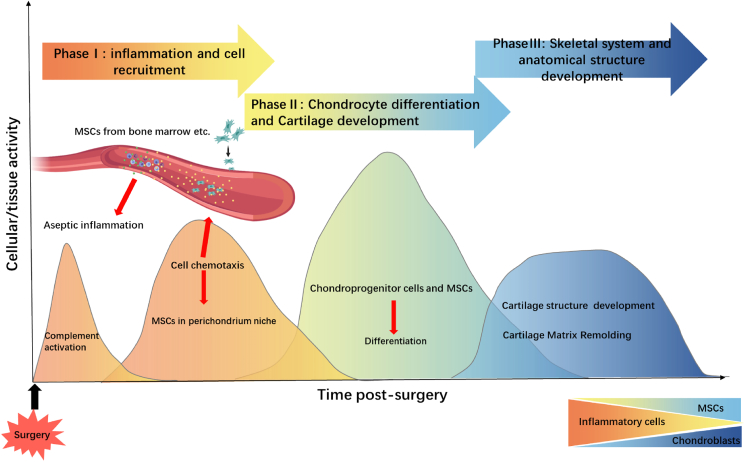
We describe a general approach to produce bone and cartilaginous structures utilizing the self-regenerative capacity of the intercostal rib space to treat a deformed metacarpophalangeal joint and microtia. Anatomically precise 3D molds were positioned on the perichondro-periosteal or perichondral flap of the intercostal rib without any other exogenous elements. We find anatomically precise metacarpal head and auricle constructs within the implanted molds after 6 months. The regenerated metacarpal head was used successfully to surgically repair the deformed metacarpophalangeal joint. Auricle reconstructive surgery in five unilateral microtia patients yielded good aesthetic and functional results. Long-term follow-up revealed the auricle constructs were safe and stable. Single-cell RNA sequencing analysis reveal early infiltration of a cell population consistent with mesenchymal stem cells, followed by IL-8-stimulated differentiation into chondrocytes. Our results demonstrate the repair and regeneration of tissues using only endogenous factors and a viable treatment strategy for bone and tissue structural defects.
Keywords: auricular reconstruction; cartilage regeneration; endogenous stem cells; joint reconstruction; regeneration medicine; tissue regeneration.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures




References
-
- Brooks P.M. The burden of musculoskeletal disease--a global perspective. Clin. Rheumatol. 2006;25:778–781. - PubMed
-
- Helmick C.G., Felson D.T., Lawrence R.C., Gabriel S., Hirsch R., Kwoh C.K., Liang M.H., Kremers H.M., Mayes M.D., Merkel P.A., et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part I. Arthritis Rheum. 2008;58:15–25. - PubMed
-
- Klein J. Chemistry. Repair or replacement--a joint perspective. Science. 2009;323:47–48. - PubMed
-
- Atala A., Bauer S.B., Soker S., Yoo J.J., Retik A.B. Tissue-engineered autologous bladders for patients needing cystoplasty. Lancet. 2006;367:1241–1246. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
