

Alcohol consumption and cancer incidence in women: interaction with smoking, body mass index and menopausal hormone therapy
- PMID: 37587405
- PMCID: PMC10428611
- DOI: 10.1186/s12885-023-11184-8
Alcohol consumption and cancer incidence in women: interaction with smoking, body mass index and menopausal hormone therapy
Abstract
Background: Alcohol consumption has been associated with increased risks of certain site-specific cancers and decreased risks of some other cancers. There is, however, little reliable evidence as to whether the alcohol-associated risks for specific cancers are modified by smoking, body mass index (BMI) and menopausal hormone therapy (MHT) use.
Methods: In the prospective UK Million Women Study, 1,233,177 postmenopausal women without prior cancer, mean age 56 (SD 5) years, reported their alcohol consumption in median year 1998 (IQR 1998-1999), and were followed by record-linkage for incident cancer. 438,056 women who drank no alcohol or < 1 drink/week were excluded. Cox regression yielded adjusted relative risks (RRs) and 95% confidence intervals (CIs) for 21 cancers by alcohol amount; statistical significance of interactions with smoking, BMI and MHT use was assessed after allowing for multiple testing.
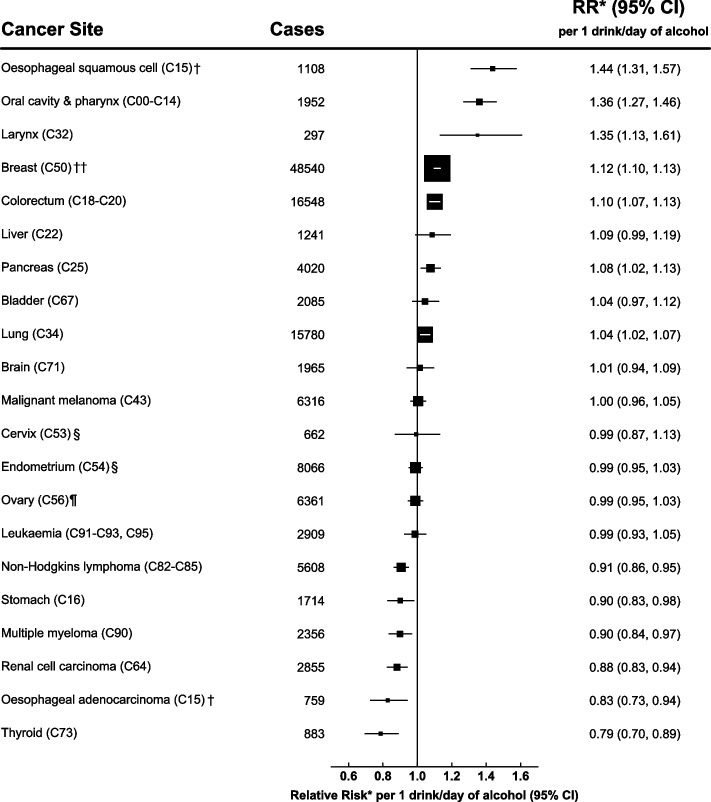
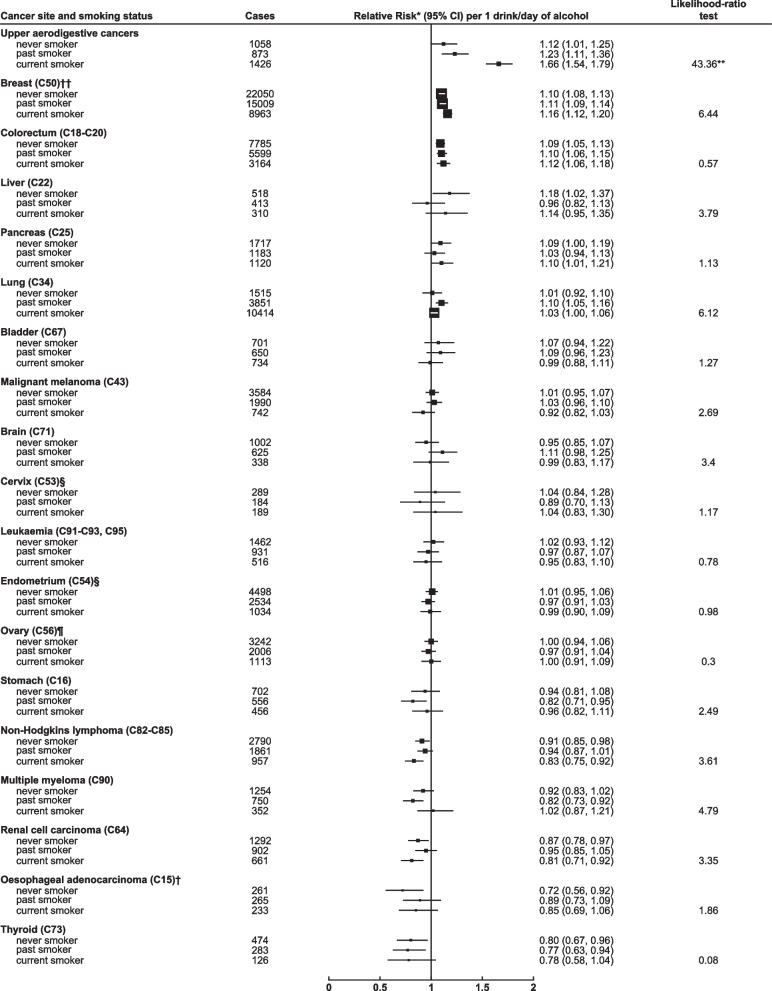
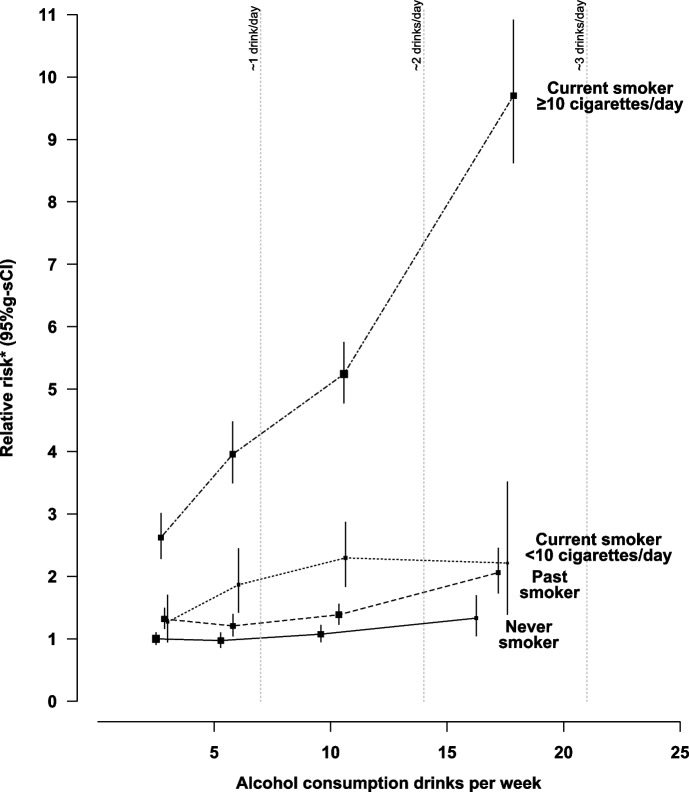
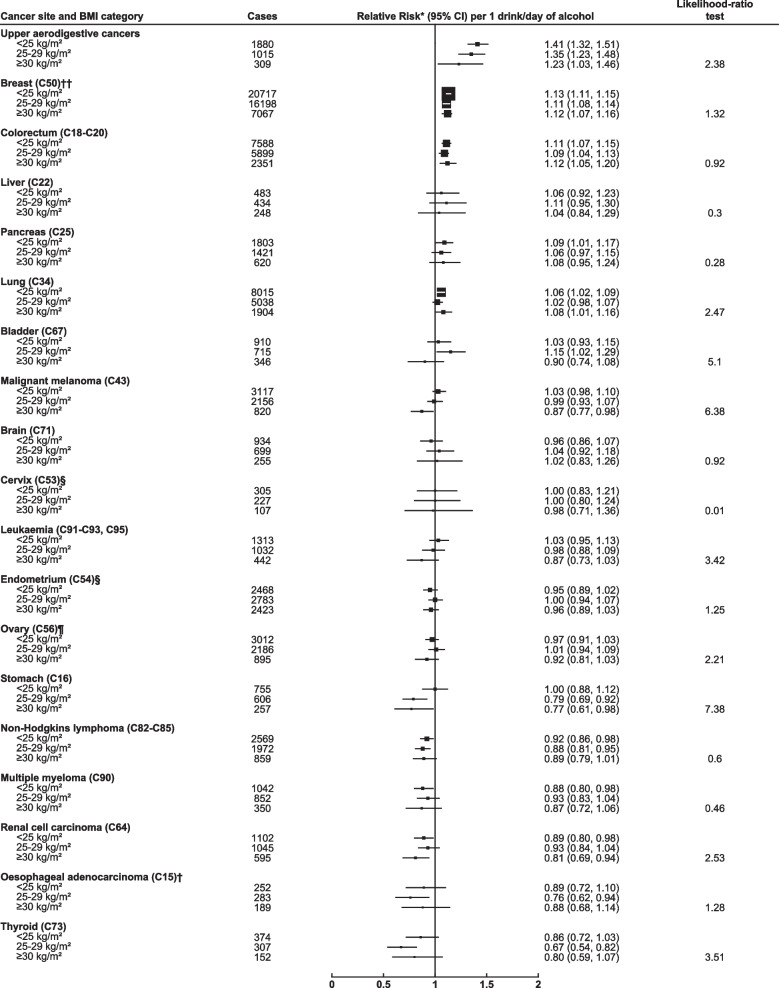
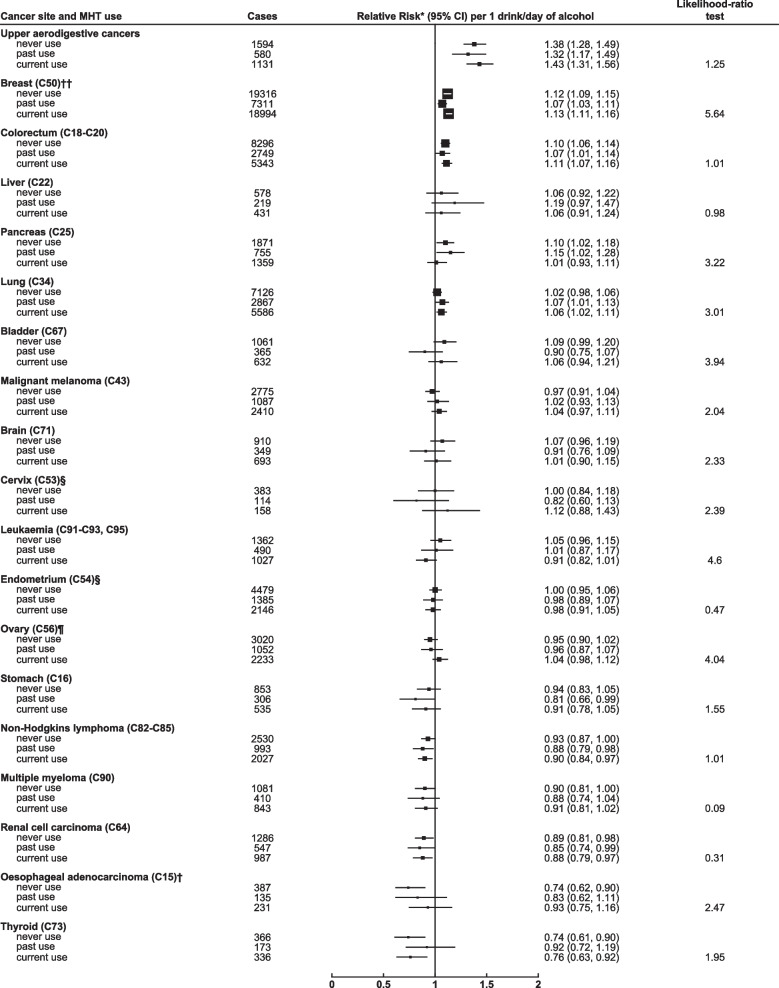
Results: In 795,121 participants, mean consumption was 6.7 (SD 6.4) alcoholic drinks/week. During 17 (SD 5) years of follow-up, 140,203 incident cancers were recorded. There was strong evidence for a substantial association between alcohol intake and risk of upper aero-digestive cancers (oesophageal squamous cell carcinoma, oral cavity, pharynx and larynx; RR per 1 drink/day = 1.38 [95% CI 1.31-1.46]). There was also strong evidence for more moderate positive associations with breast, colorectal and pancreatic cancer (RRs per 1 drink/day = 1.12 [1.10-1.14], 1.10 [1.07-1.13], 1.08 [1.02-1.13] respectively), and moderate negative associations with thyroid cancer, non-Hodgkin's lymphoma, renal cell carcinoma and multiple myeloma (RRs per 1 drink/day = 0.79 [0.70-0.89], 0.91 [0.86-0.95], 0.88 [0.83-0.94], 0.90 [0.84-0.97] respectively). Significant interactions between alcohol and smoking were seen for upper aero-digestive cancers (RRs per 1 drink/day = 1.66 [1.54-1.79], 1.23 [1.11-1.36], 1.12 [1.01-1.25] in current, past, and never smokers respectively). BMI and MHT did not significantly modify any alcohol-associated risks.
Conclusions: These findings provide robust evidence that greater alcohol intake, even within relatively moderate ranges, increases the risk of cancers of the aerodigestive tract, breast, colorectal and pancreatic cancer, and probably decreases the risk of thyroid cancer, non-Hodgkin's lymphoma, renal cell carcinoma and multiple myeloma. Associations of alcohol intake with cancer risk were not modified by MHT use, adiposity or smoking, except in the case of upper aero-digestive cancers, where the alcohol-associated risk was largely confined to smokers.
Keywords: Alcohol; Cancer; Epidemiology.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Wild CP, Weiderpass E, Stewart BW, editors. World Cancer Report: Cancer Research for Cancer Prevention. Lyon,. Lyon, France: International Agency for Research on Cancer. 2020. Available from: http://publications.iarc.fr/586.
-
- Endogenous Hormones Breast Cancer Collaborative Group. Key TJ, Appleby PN, Reeves GK, Roddam AW, Helzlsouer KJ, et al. Circulating sex hormones and breast cancer risk factors in postmenopausal women: reanalysis of 13 studies. Br J Cancer. 2011;105(5):709–22. doi: 10.1038/bjc.2011.254. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
