

The use of the CNIC-Polypill in real-life clinical practice: opportunities and challenges in patients at very high risk of atherosclerotic cardiovascular disease - expert panel meeting report
- PMID: 37587509
- PMCID: PMC10433542
- DOI: 10.1186/s12919-023-00268-9
The use of the CNIC-Polypill in real-life clinical practice: opportunities and challenges in patients at very high risk of atherosclerotic cardiovascular disease - expert panel meeting report
Erratum in
-
Correction: The use of the CNIC-Polypill in real-life clinical practice: opportunities and challenges in patients at very high risk of atherosclerotic cardiovascular disease - expert panel meeting report.BMC Proc. 2023 Oct 12;17(1):27. doi: 10.1186/s12919-023-00279-6. BMC Proc. 2023. PMID: 37828604 Free PMC article. No abstract available.
Abstract
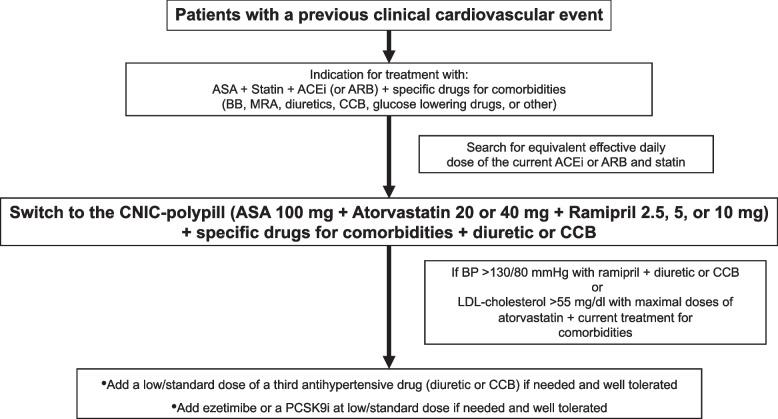
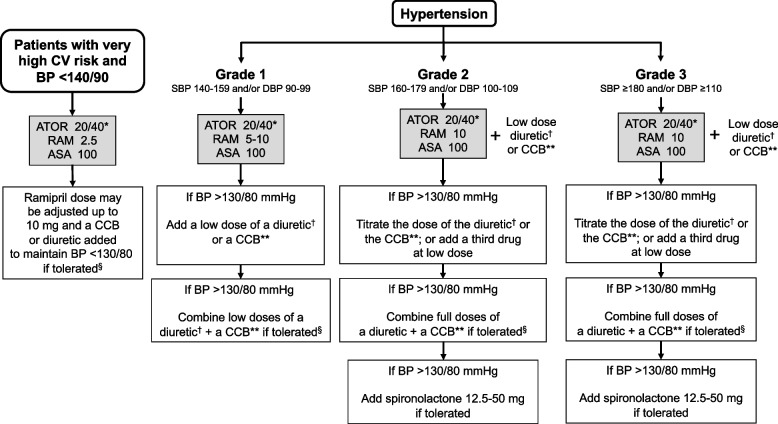
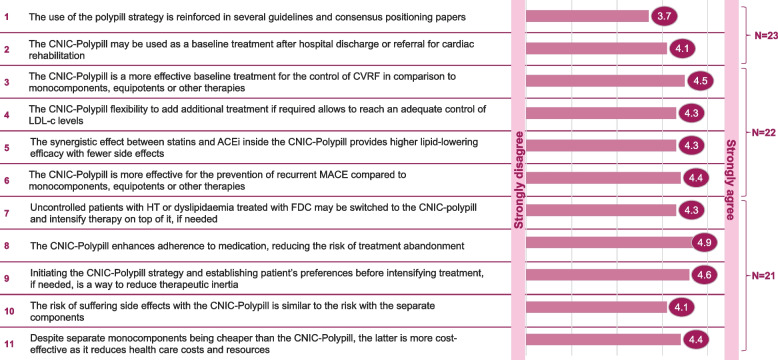
Although the cardiovascular (CV) polypill concept is not new and several guidelines state that a CV polypill should be considered an integral part of a comprehensive CV disease (CVD) prevention strategy, there are still some barriers to its implementation in the real-world setting, mainly in secondary CV prevention. As the CNIC-polypill is the only one approved for secondary CV prevention in patients with atherosclerotic CVD in 27 countries worldwide, a panel of four discussants and 30 participants from 18 countries conveyed in a virtual meeting on April 21, 2022, to discuss key clinical questions regarding the practical use of the CNIC-Polypill and barriers to its implementation.Data presented showed that, although the use of the CV polypill is not explicitly mentioned in the current 2021 European Society of Cardiology guidelines on CVD prevention, it may be used in any patient for secondary CVD prevention tolerating all their components to improve outcomes through different aspects. The favourable results of the Secondary Prevention of Cardiovascular Disease in the Elderly (SECURE) trial now reinforce this recommendation. The panellists presented algorithms on how to switch from any baseline regimen when starting treatment with the CNIC-polypill in different situations, including patients with hypertension, dyslipidaemia, and a previous CV event; at discharge after a cardiovascular event; in chronic ischemic conditions; and in cases of polypharmacy. The panellists and expert discussants did agree that available studies conducted so far with the CNIC-polypill demonstrate that it is as efficacious as the monocomponents, equipotent drugs, or other therapies; reduces the risk of experiencing recurrent major CV events; improves medication adherence; reduces health care costs and resources compared to patients treated with loose drugs; and the patients prefer it over the multipill strategy.In conclusion, the data presented by the participants provided the evidence behind the use of the CNIC-polypill to help fulfil the goal of encouraging its adoption by physicians.
Keywords: Cardiovascular disease; Cerebrovascular disease; Fixed-dose combination; Polypill; Secondary prevention.
© 2023. The Author(s).
Conflict of interest statement
LG-S has no competing interests to declare. AC has received honoraria for lectures in symposia and educational activities sponsored by unrestricted grants from Abbott, Berlin-Chemie, Biolab, Boehringer, Ferrer, Menarini, Merck, and Sanofi. JM has received honoraria for lectures in symposia and educational activities sponsored by unrestricted grants from, Astra Zeneca, Bayer, Novartis, Menarini, and Servier. PP-M has received fees for lectures and educational activities from Novo-Nordisk, Boehringer Ingelheim, Amgen, Laboratorios Dr Esteve, MSD, Ferrer, Menarini, Servier, and Viatrix.
Figures




References
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2018;39:119–177. doi: 10.1093/eurheartj/ehx393. - DOI - PubMed
-
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens. 2018;36:1953–2041. doi: 10.1097/HJH.0000000000001940. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
