

Humerus shaft fractures, approaches and management
- PMID: 37588079
- PMCID: PMC10425411
- DOI: 10.1016/j.jcot.2023.102230
Humerus shaft fractures, approaches and management
Abstract
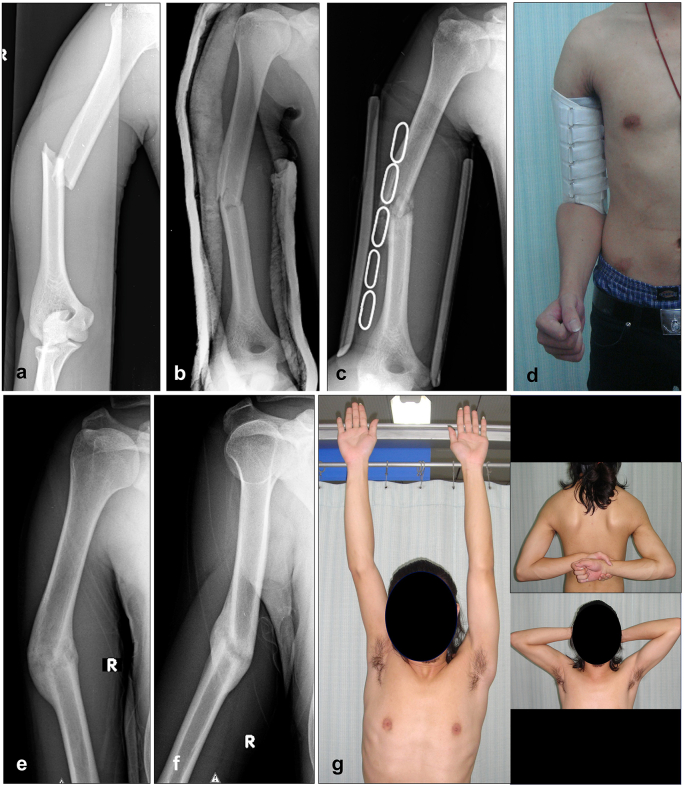
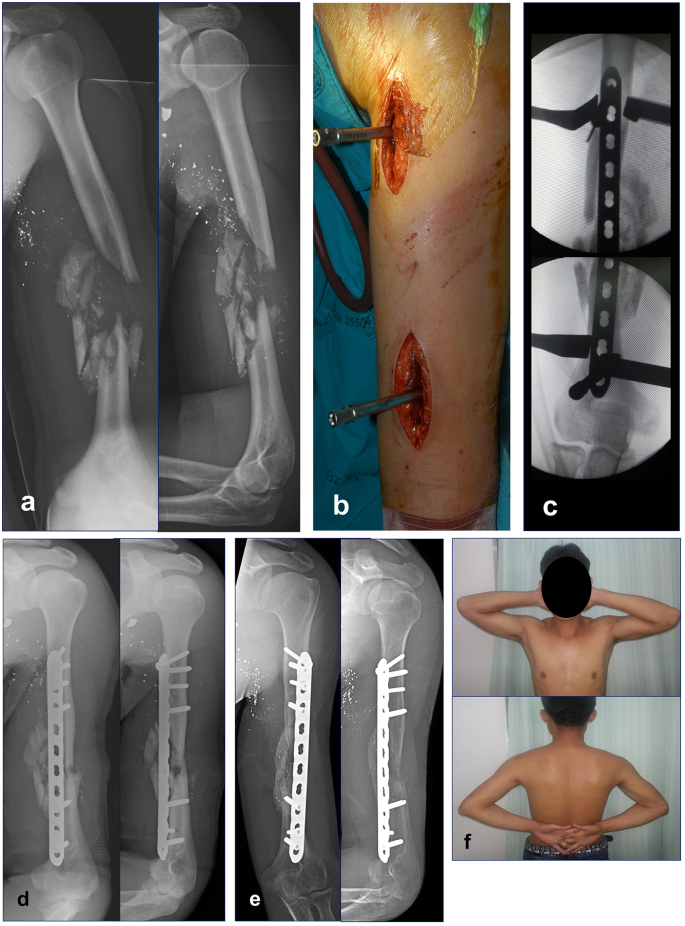
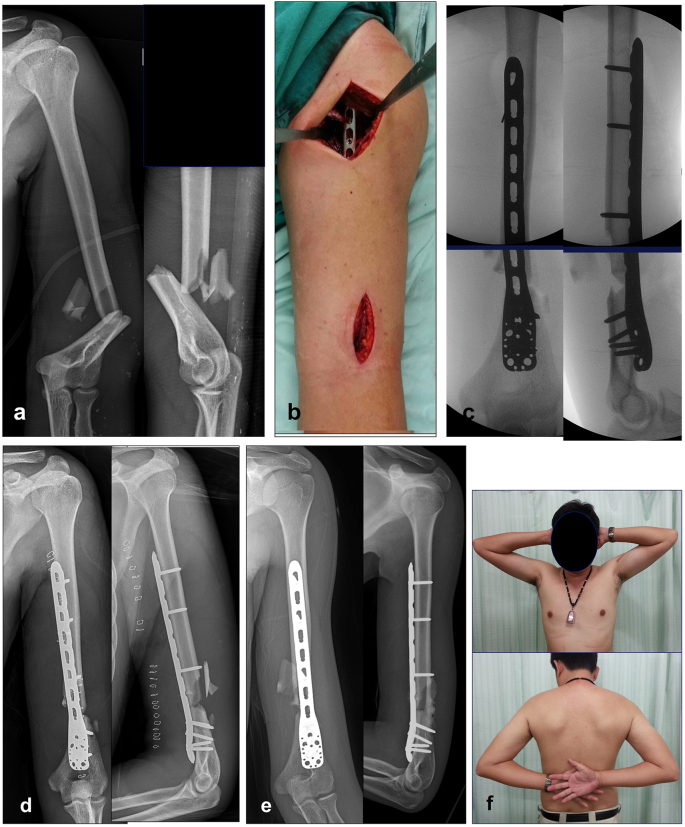
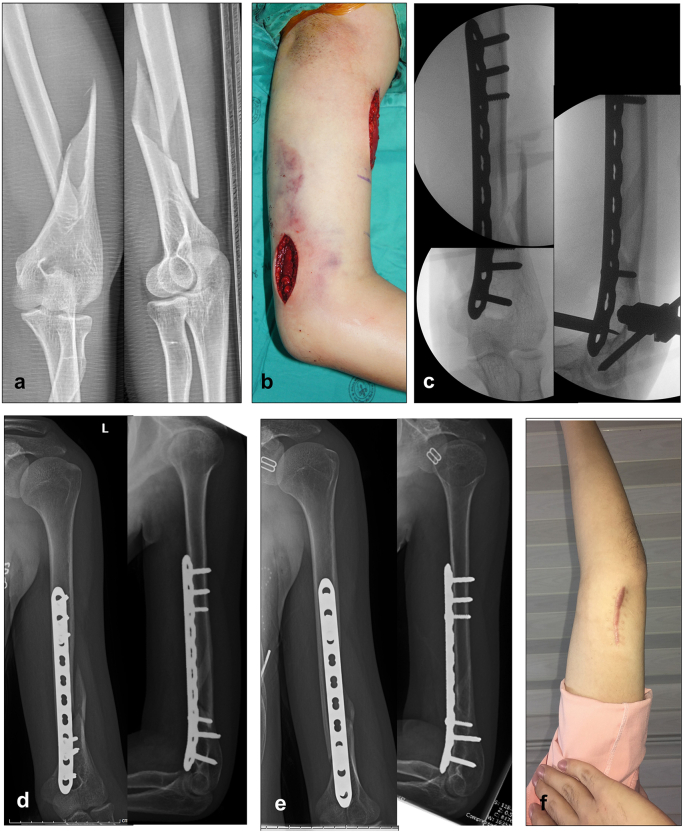
Humeral shaft fracture is a common injury which can be treated either conservatively with functional bracing or with surgical fixation. Current evidence shows an increase in the rate of nonunion after conservative treatment, suggesting that indications for conservative treatment may need to be re-examined. This article updates trends in treatment for humeral shaft fracture. Indications for surgery, both for plate osteosynthesis with open reduction and internal fixation (ORIF) as well as for minimally invasive plate osteosynthesis (MIPO) and intramedullary nailing (IMN) are described. Recognition of the advantages and disadvantages of each technique can better define the role of the plate or nail and can aid in the selection of an appropriate surgical approach. ORIF with compression plate continues to have a role in the treatment of simple or AO/OTA type A fractures. The primary goal of minimal invasive osteosynthesis, a surgical technique involving small incisions, closed reduction or mini-open reduction that minimizes soft tissue dissection and helps preserve the periosteal blood supply, is to achieve bone union and the best possible functional outcomes. MIPO of the humerus is now well accepted as being less invasive and providing relative stability to allow indirect (secondary) bone healing with callus formation. MIPO approaches can be performed circumferentially to the humerus, including the proximal, middle and distal shaft. The classic MIPO approach is anterior MIPO, followed by posterior, anterolateral and anteromedial MIPO. IMN is also an option for treating humerus fractures. In the past, IMN was not widely used due to the potential for complications such as shoulder impingement and elbow problems as well as the limited availability of implants and the steep learning curve of this surgical technique. Over the past decade, the launch of a new design of straight antegrade and retrograde IMN with established techniques has encouraged more surgeons to use IMN as an alternative option. Methods of dealing with concomitant and post-treatment radial nerve palsy have also been evolving, including the use of ultrasound for diagnosis of radial nerve conditions. Radial nerves with contusion, entrapment or laceration can be detected using ultrasound with reliability comparable to intraoperative findings. Trends in treatment of radial nerve palsy are described below. Future larger randomized controlled trials comparing conservative and operative management are necessary to further develop appropriate guidelines.
Keywords: Conservative; Fracture; Humeral shaft; Intramedullary nailing; MIPO; ORIF; Radial nerve injury; Treatment; Ultrasound.
© 2023 Delhi Orthopedic Association. All rights reserved.
Conflict of interest statement
The authors do not received funding from any source. We received no payments or other benefits from any commercial entity.
Figures

References
-
- Lode I., et al. Operative versus nonoperative treatment of humeral shaft fractures: a systematic review and meta-analysis. J Shoulder Elbow Surg. 2020;29(12):2495–2504. - PubMed
-
- Oliver W.M., et al. Surgical versus nonsurgical management of humeral shaft fractures: a systematic review and meta-analysis of randomized trials. J Am Acad Orthop Surg. 2023;31(2):e82–e93. - PubMed
-
- Sarmiento A., et al. Functional bracing of fractures of the shaft of the humerus. J Bone Joint Surg Am. 1977;59(5):596–601. - PubMed
-
- Serrano R., et al. Modern results of functional bracing of humeral shaft fractures: a multicenter retrospective analysis. J Orthop Trauma. 2020;34(4):206–209. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous