

Elbow lateral ulnar collateral ligament reconstruction by transposition of the local extensor fascia septum: surgical technique and preliminary results
- PMID: 37588856
- PMCID: PMC10426691
- DOI: 10.1016/j.xrrt.2022.04.004
Elbow lateral ulnar collateral ligament reconstruction by transposition of the local extensor fascia septum: surgical technique and preliminary results
Abstract
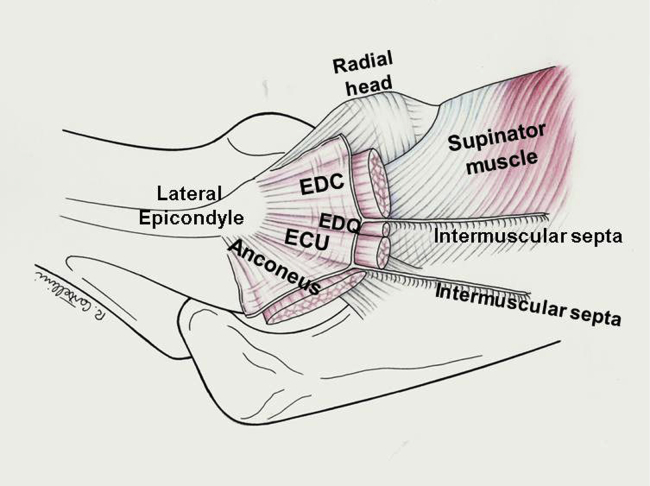
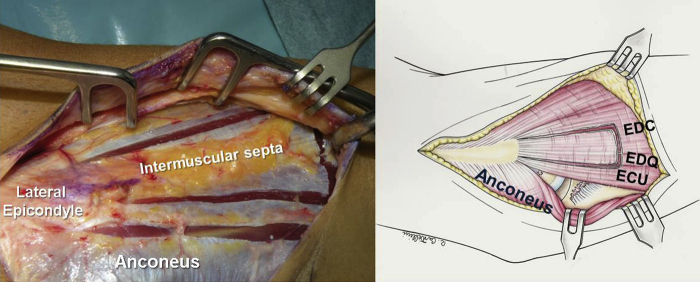
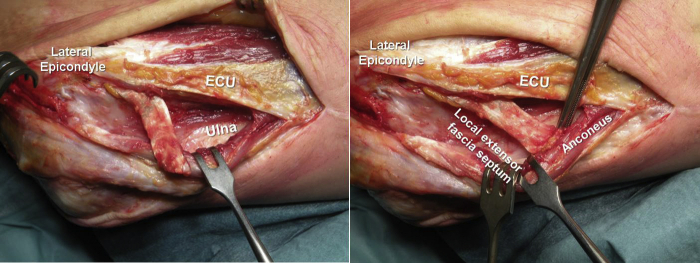
The lateral ulnar collateral ligament (LUCL) is a primary lateral stabilizer of the elbow that originates from the isometric center of the capitulum and inserts into the supinator crest of the ulna. LUCL injury may be due to trauma, chronic strain, or iatrogenic lesion. In patients with symptomatic LUCL insufficiency and recurrent posterolateral rotatory instability, surgical reconstruction can restore elbow stability. In primary acute treatment, the injured LUCL is reattached to the lateral epicondyle with transosseous sutures and anchors placed at the isometric origin of the ligament. If the ligament quality is poor, patients with chronic elbow instability may require reconstruction with a tendon autograft or allograft. Alternatively, the LUCL can be reconstructed by transposition of the local extensor fascia septum, a local flap that exploits the common extensor fascia connected to a thin strip of extensor digitorum quinti or the extensor digitorum communis intermuscular septum. We describe a new LUCL reconstruction technique based on the transposition of the local extensor fascia septum and report the preliminary result in a series of patients aged 50 years or less.
Keywords: Chronic strain; Iatrogenic lesion; Lateral ulnar collateral ligament; Soft tissue lesions; Transposition of the local extensor fascia septum; Trauma.
© 2022 The Author(s).
Figures











References
-
- Badhrinarayanan S., Desai A., Watson J.J., White C.H.R., Phadnis J. Indications, Outcomes, and Complications of Lateral Ulnar Collateral Ligament Reconstruction of the Elbow for Chronic Posterolateral Rotatory Instability: A Systematic Review. Am J Sports Med. 2021;49:830–837. doi: 10.1177/0363546520927412. - DOI - PubMed
-
- Cohen M.S., Hastings H.H. Rotatory instability of the elbow, the anatomy and role of the lateral stabilizers. J Bone Joint Surg Am. 1997;79:225–233. - PubMed
LinkOut - more resources
Full Text Sources
