

Ventricular arrhythmias recorded on 12-lead ambulatory electrocardiogram monitoring in healthy volunteer athletes and controls: what is common and what is not
- PMID: 37589170
- PMCID: PMC10469403
- DOI: 10.1093/europace/euad255
Ventricular arrhythmias recorded on 12-lead ambulatory electrocardiogram monitoring in healthy volunteer athletes and controls: what is common and what is not
Abstract
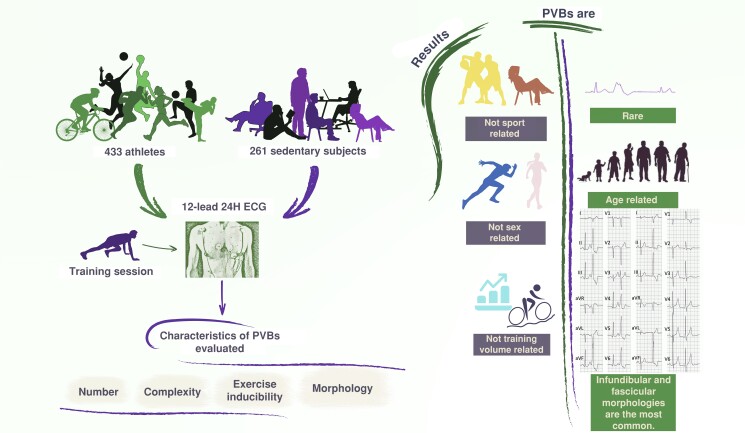
Aims: Premature ventricular beats (PVBs) in athletes are often benign, but sometimes they may be a sign of an underlying disease. We evaluated the prevalence, burden, and morphology of PVBs in healthy voluntary athletes and controls with the main purpose of defining if certain PVB patterns are 'common' and 'training related' and, as such, are more likely benign.
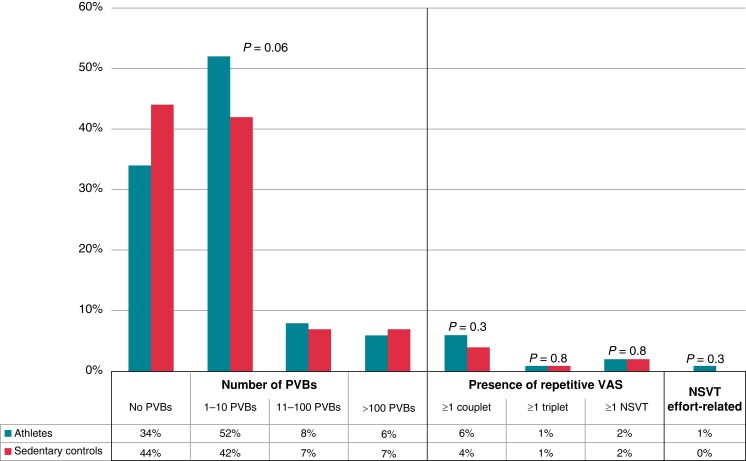
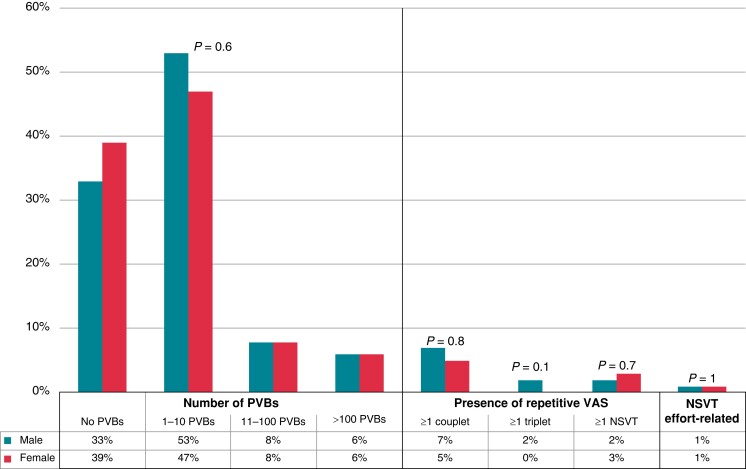
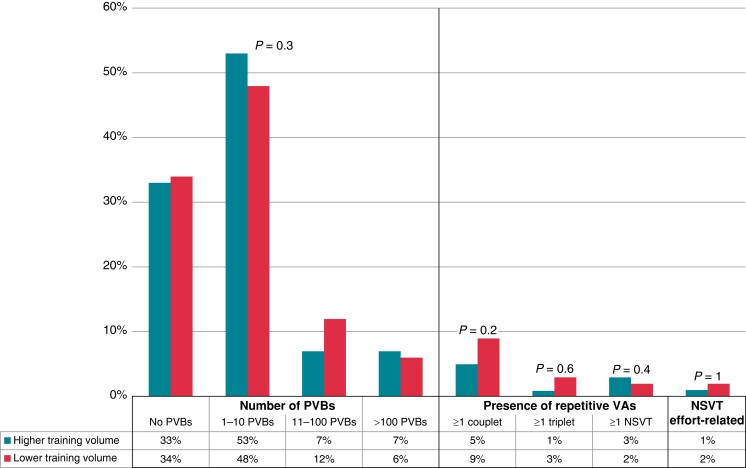
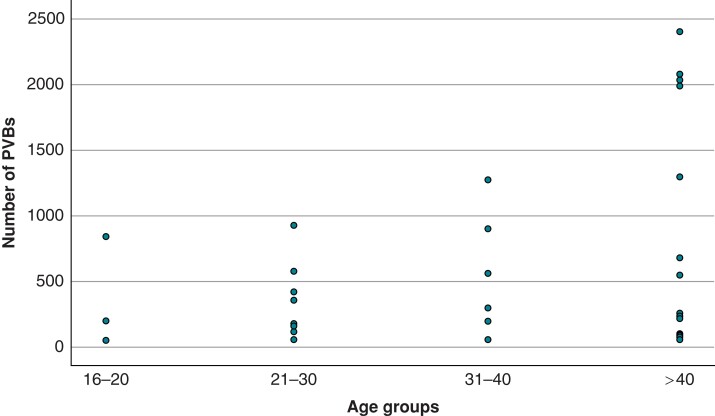
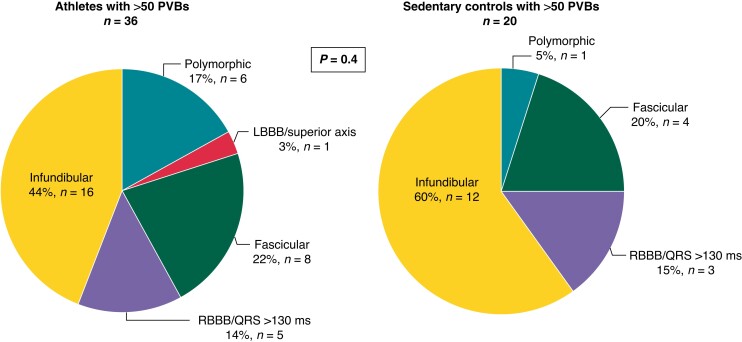
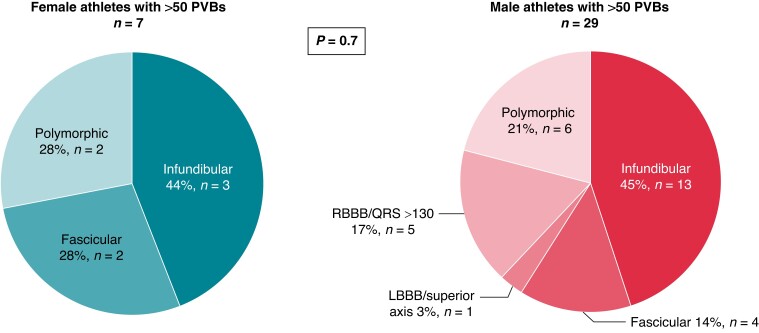
Methods and results: We studied 433 healthy competitive athletes [median age 27 (18-43) years, 74% males] and 261 age- and sex-matched sedentary subjects who volunteered to undergo 12-lead 24 h ambulatory electrocardiogram (ECG) monitoring (24H ECG), with a training session in athletes. Ventricular arrhythmias (VAs) were evaluated in terms of their number, complexity [i.e. couplet, triplet, or non-sustained ventricular tachycardia (NSVT)], exercise inducibility, and morphology. Eighty-six percent of athletes and controls exhibited a total of ≤10 PVBs/24 h, and >90% did not show any couplets, triplets, or runs of NSVT > 3 beats. An higher number of PVBs correlated with increasing age (P < 0.01) but not with sex and level of training. The most frequent morphologies among the 36 athletes with >50 PVBs were the infundibular (44%) and fascicular (22%) ones. In a comparison between athletes and sedentary individuals, and male and female athletes, no statistically significant differences were found in PVBs morphologies.
Conclusion: The prevalence and complexity of VAs at 24H ECG did not differ between athletes and sedentary controls and were not related to the type and amount of sport or sex. Age was the only variable associated with an increased PVB burden. Thus, no PVB pattern in the athlete can be considered 'common' or 'training related'.
Keywords: Pre-participation screening; Premature ventricular beats; Sports cardiology; Sudden cardiac death; Ventricular arrhythmias.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
References
-
- Hingorani P, Karnad DR, Rohekar P, Kerkar V, Lokhandwala YY, Kothari S. Arrhythmias seen in baseline 24-hour Holter ECG recordings in healthy normal volunteers during phase 1 clinical trials. J Clin Pharmacol 2016;56:885–93. - PubMed
-
- von Rotz M, Aeschbacher S, Bossard M, Schoen T, Blum S, Schneider Set al. Risk factors for premature ventricular contractions in young and healthy adults. Heart 2017;103:702–7. - PubMed
-
- Biffi A, Maron BJ, Verdile L, Fernando F, Spataro A, Marcello Get al. Impact of physical deconditioning on ventricular tachyarrhythmias in trained athletes. J Am Coll Cardiol 2004;44:1053–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
