

Systematic review with meta-analysis: Medical therapies for treatment of ulcerative proctitis
- PMID: 37589498
- PMCID: PMC11162959
- DOI: 10.1111/apt.17666
Systematic review with meta-analysis: Medical therapies for treatment of ulcerative proctitis
Abstract
Background: Ulcerative proctitis (UP) is a common highly symptomatic form of ulcerative colitis that can be difficult to treat.
Aim: To assess the efficacy of medical treatments for UP.
Methods: We searched MEDLINE, EMBASE, and CENTRAL on 23 November 2022 for randomised controlled trials (RCTs) of medical therapy for adults with UP. Primary outcomes included induction and maintenance of clinical remission. Pooled risk ratios (RRs) and 95% confidence intervals (CIs) were calculated for each outcome.
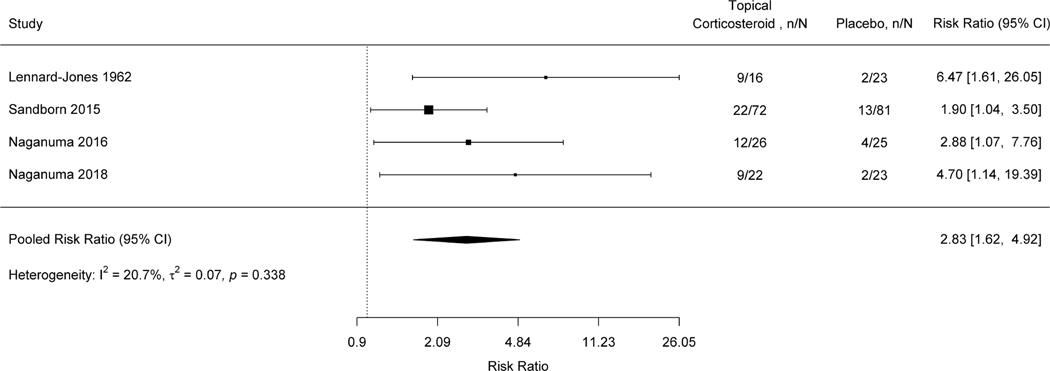
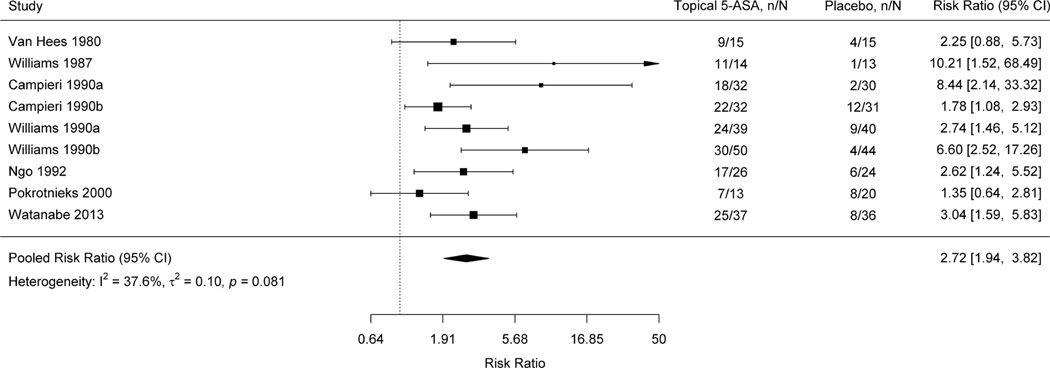
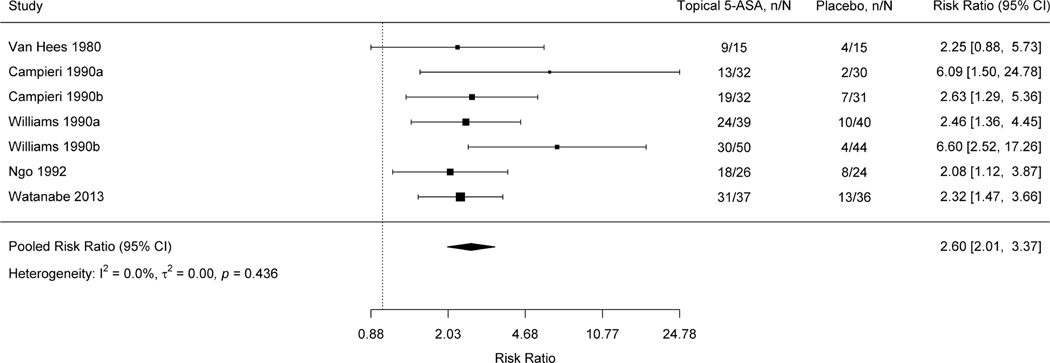
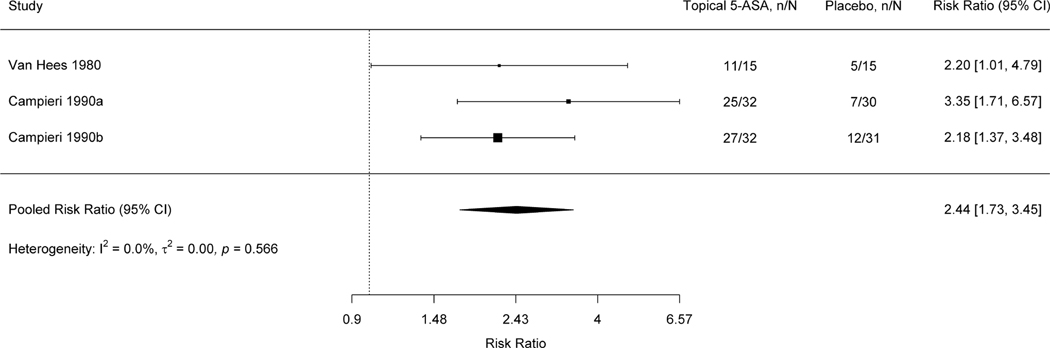
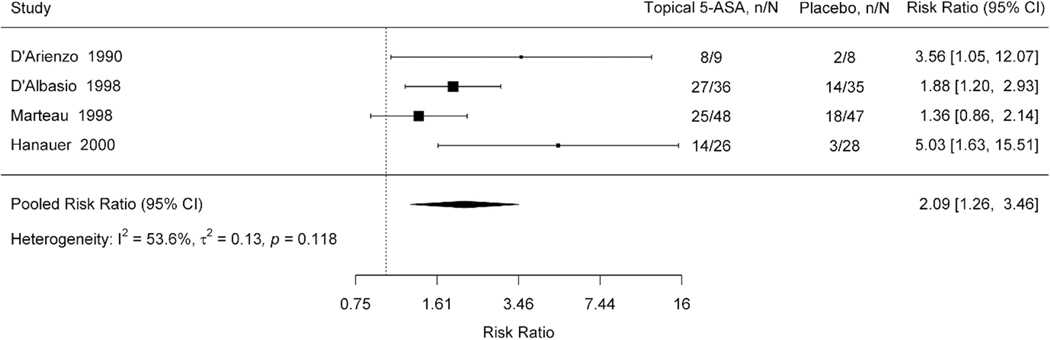
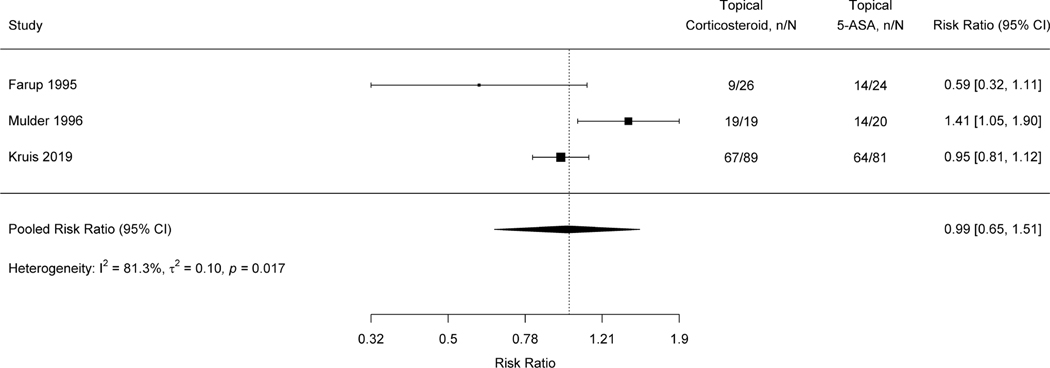
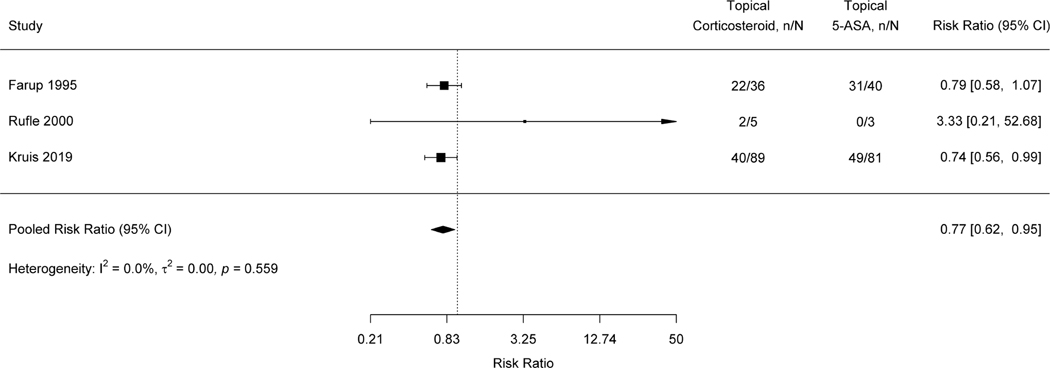
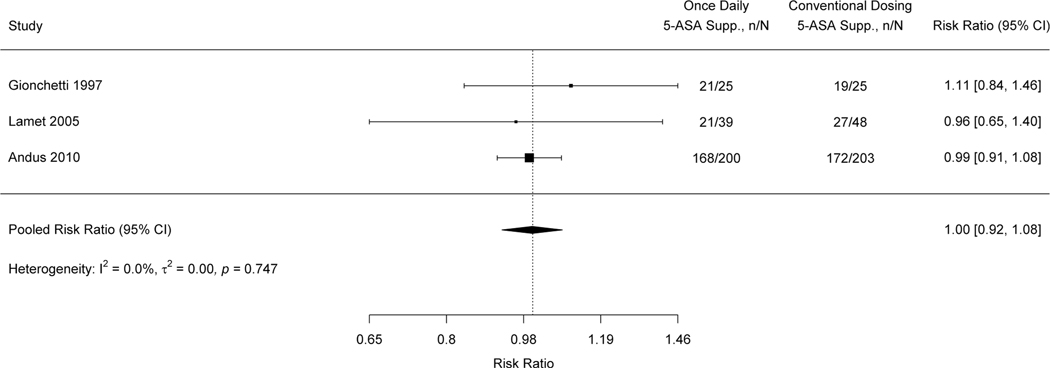
Results: We included 53 RCTs (n = 4096) including 46 induction studies (n = 3731) and seven maintenance studies (n = 365). First-line therapies included topical 5-aminosalicylic acid (5-ASA), conventional corticosteroids, budesonide, and oral 5-ASA. Therapy for refractory UP included topical tacrolimus and small molecules. Topical 5-ASA was superior to placebo for induction (RR 2.72, 95% CI 1.94-3.82) and maintenance of remission (RR 2.09, 95% CI 1.26-3.46). Topical corticosteroids were superior to placebo for induction of remission (RR 2.83, 95% CI 1.62-4.92). Topical budesonide was superior to placebo for induction of remission (RR 2.34, 95% CI 1.44-3.81). Combination therapy with topical 5-ASA and topical corticosteroids was superior to topical monotherapy with either agent. Topical tacrolimus was superior to placebo. Etrasimod was superior to placebo for induction (RR 4.71, 95% CI 1.2-18.49) and maintenance of remission (RR 2.08, 95% CI 1.31-3.32).
Conclusions: Topical 5-ASA and corticosteroids are effective for active UP. Topical 5-ASA may be effective for maintenance of remission. Tacrolimus may be effective for induction of remission. Etrasimod may be effective for induction and for maintenance of remission. Trials should include UP to expand the evidence base for this under-represented population.
© 2023 John Wiley & Sons Ltd.
Conflict of interest statement
Figures

References
-
- van den Heuvel TR, Jeuring SF, Zeegers MP, van Dongen D, Wolters A, Masclee AAM, et al. A 20-year temporal change analysis in incidence, presenting phenotype and mortality, in the Dutch IBDSL cohort—can diagnostic factors explain the increase in IBD incidence? J Crohn's Colitis. 2017;11(10):1169–79. - PubMed
-
- Meucci G, Vecchi M, Astegiano M, Beretta L, Cesari P, Dizioli P, et al. The natural history of ulcerative proctitis: a multicenter, retrospective study. Am J Gastroenterol. 2000;95(2):469–73. - PubMed
-
- Hochart A, Gower-Rousseau C, Sarter H, Fumery M, Ley D, Spyckerelle C, et al. Ulcerative proctitis is a frequent location of paediatric-onset UC and not a minor disease: a population-based study. Gut. 2017;66(11):1912–7. - PubMed
-
- Kruis W, Brandes J, Schreiber S, Theuer D, Krakamp B, Schütz E, et al. Olsalazine versus mesalazine in the treatment of mild to moderate ulcerative colitis. Aliment Pharmacol Ther. 1998;12(8):707–15. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical