

Bronchial branching patterns and volumetry in the right upper lobe: impact on segmentectomy planning
- PMID: 37589657
- PMCID: PMC10702455
- DOI: 10.1093/icvts/ivad136
Bronchial branching patterns and volumetry in the right upper lobe: impact on segmentectomy planning
Abstract
Objectives: The use of segmentectomy is expected to increase. However, understanding of the segmental bronchial branching is limited. Herein, we aimed to investigate bronchial branching pattern complexity and segmental volumetry of the right upper lung lobe to develop an accurate understanding of segmental anatomy and contribute to the advancement of safe and efficient lung segmentectomy.
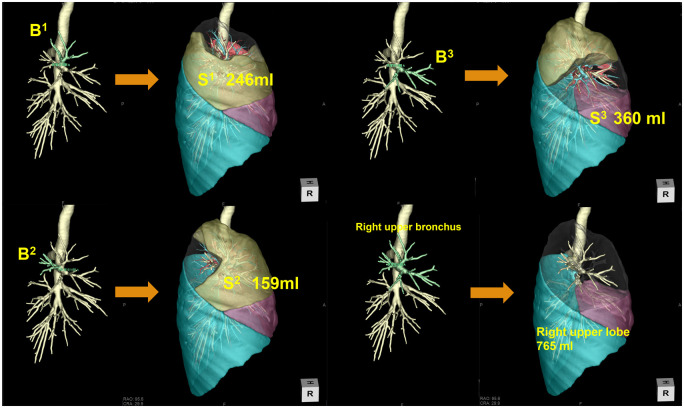
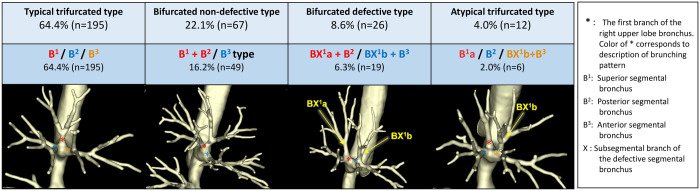
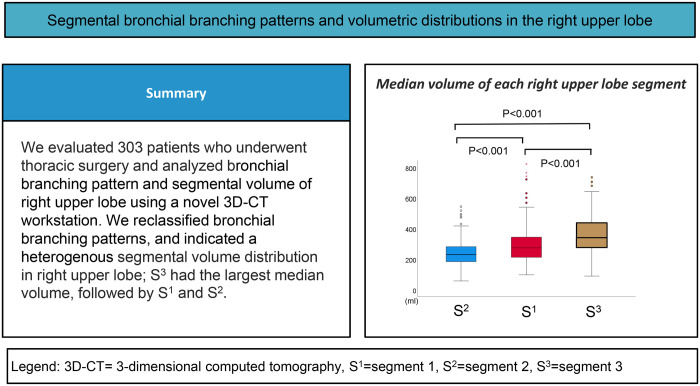
Methods: We evaluated chest computed tomography scans of 303 patients and categorized the branching of segmental bronchi (segment 1, apical; segment 2, posterior; and segment 3, anterior) into 4 major types (typical trifurcated, bifurcated non-defective, bifurcated defective and atypical trifurcated) and 11 subtypes. Segmental volumetry was performed to determine the predominant segment in each case (volume difference <5% was considered equal). Branching complexity was evaluated separately for volumetry-predominant and volumetry-non-predominant segments.
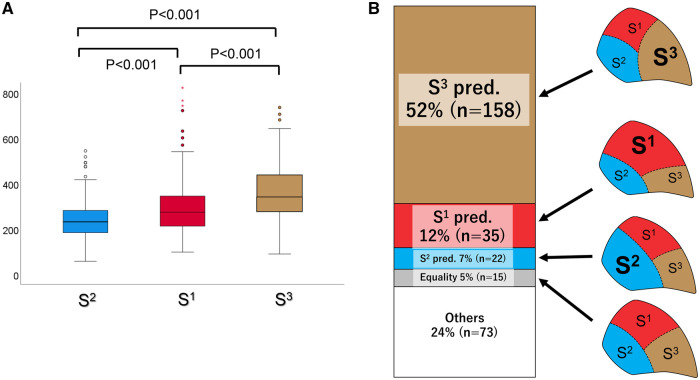
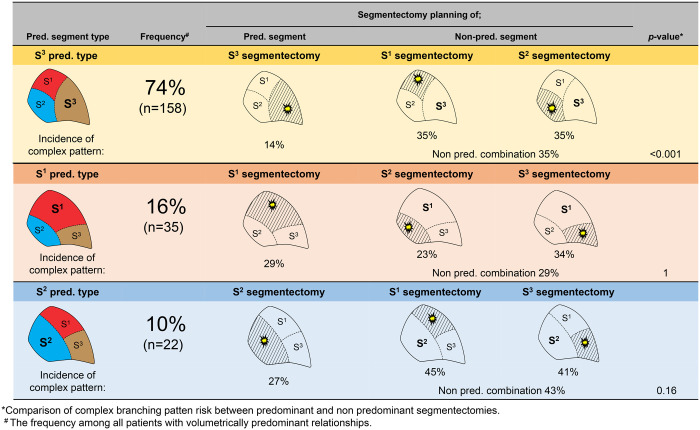
Results: Trifurcated non-defective was the most frequent branching type (64.4%), followed by bifurcated non-defective (22.1%), bifurcated defective (8.6%) and trifurcated half-defective (4.0%). In terms of segmental volumetry, most cases had a one-segment-predominant distribution (71%) and only 5% of cases had equal distribution (segment 1 = segment 2 = segment 3). More than half of the cases had a segment 3-predominant distribution (52%). Branching complexity analysis revealed that the volumetry-non-predominant segment was associated with a higher risk of complex branching patterns compared with the volumetry-predominant segment (37% vs 19%, respectively; P < 0.005).
Conclusions: Volumetric assessment of the right upper lobe showed a heterogeneous segmental volume distribution. Care should be taken during lung segmentectomy of the volumetry-non-predominant segments because of the high risk associated with complex bronchial branching patterns.
Clinical trial registration: No. 4840.
Keywords: Bronchial branching pattern; Pulmonary segmentectomy; Right upper lobe; Volumetry.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
References
-
- Okada M, Koike T, Higashiyama M, Yamato Y, Kodama K, Tsubota N.. Radical sublobar resection for small-sized non-small cell lung cancer: a multicenter study. J Thorac Cardiovasc Surg 2006;132:769–75. - PubMed
-
- Harada H, Okada M, Sakamoto T, Matsuoka H, Tsubota N.. Functional advantage after radical segmentectomy versus lobectomy for lung cancer. Ann Thorac Surg 2005;80:2041–5. - PubMed
-
- Keenan RJ, Landreneau RJ, Maley RH Jr, Singh D, Macherey R, Bartley S. et al. Segmental resection spares pulmonary function in patients with stage I lung cancer. Ann Thorac Surg 2004;78:228–33; discussion 228–33. - PubMed
-
- Ohtaki Y, Shimizu K.. Anatomical thoracoscopic segmentectomy for lung cancer. Gen Thorac Cardiovasc Surg 2014;62:586–93. - PubMed
-
- Nakazawa S, Shimizu K, Mogi A, Kuwano H.. VATS segmentectomy: past, present, and future. Gen Thorac Cardiovasc Surg 2018;66:81–90. - PubMed
LinkOut - more resources
Full Text Sources
