

Obesity dominates early effects on cardiac structure and arterial stiffness in people with type 2 diabetes
- PMID: 37589719
- PMCID: PMC10592255
- DOI: 10.1097/HJH.0000000000003534
Obesity dominates early effects on cardiac structure and arterial stiffness in people with type 2 diabetes
Abstract
Objective: Type 2 diabetes (T2D) and obesity are global epidemics leading to excess cardiovascular disease (CVD). This study investigates standard and novel cardiac MRI parameters to detect subclinical cardiac and central vascular dysfunction in inactive people with and without T2D.
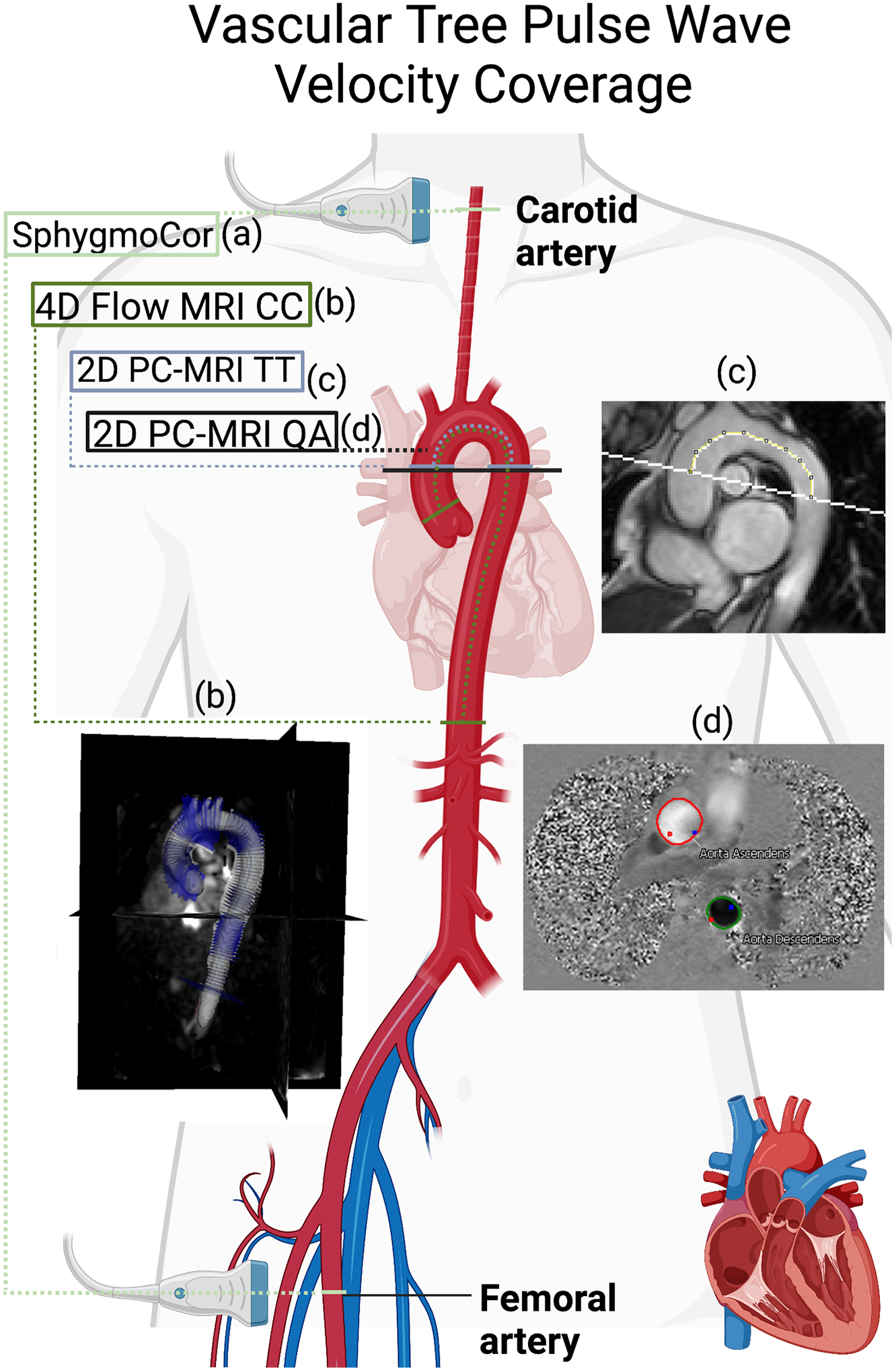
Methods: Physically inactive age and BMI-similar premenopausal women and men with ( n = 22) and without [ n = 34, controls with overweight/obesity (CWO)] uncomplicated T2D were compared to an age-similar and sex-similar reference control cohort ( n = 20). Left ventricular (LV) structure, function, and aortic stiffness were assessed by MRI. Global arterial pulse wave velocity (PWV) was assessed using carotid-to-femoral applanation tonometry. Regional PWV was measured via 2D phase-contrast MRI and 4D flow MRI.
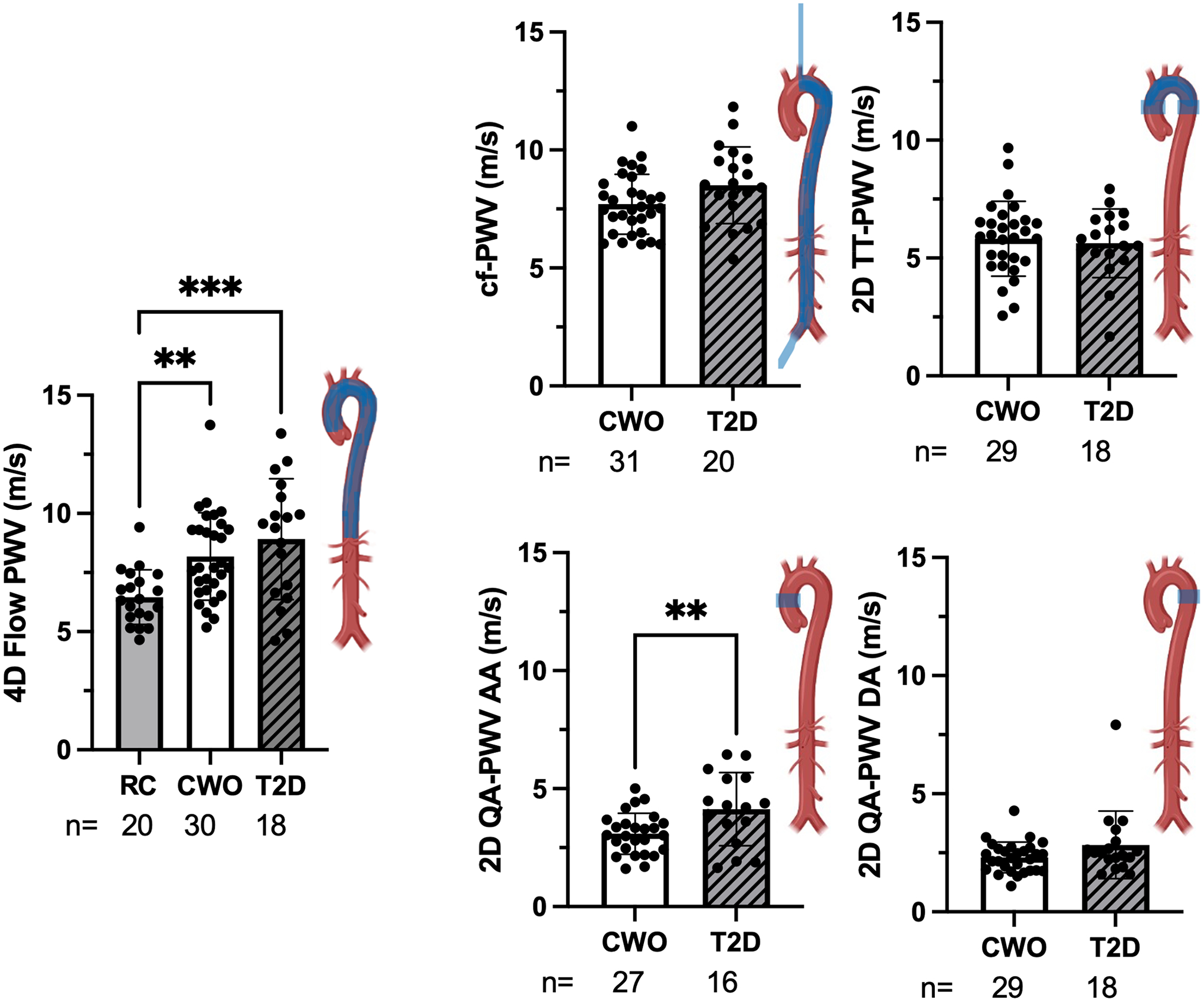
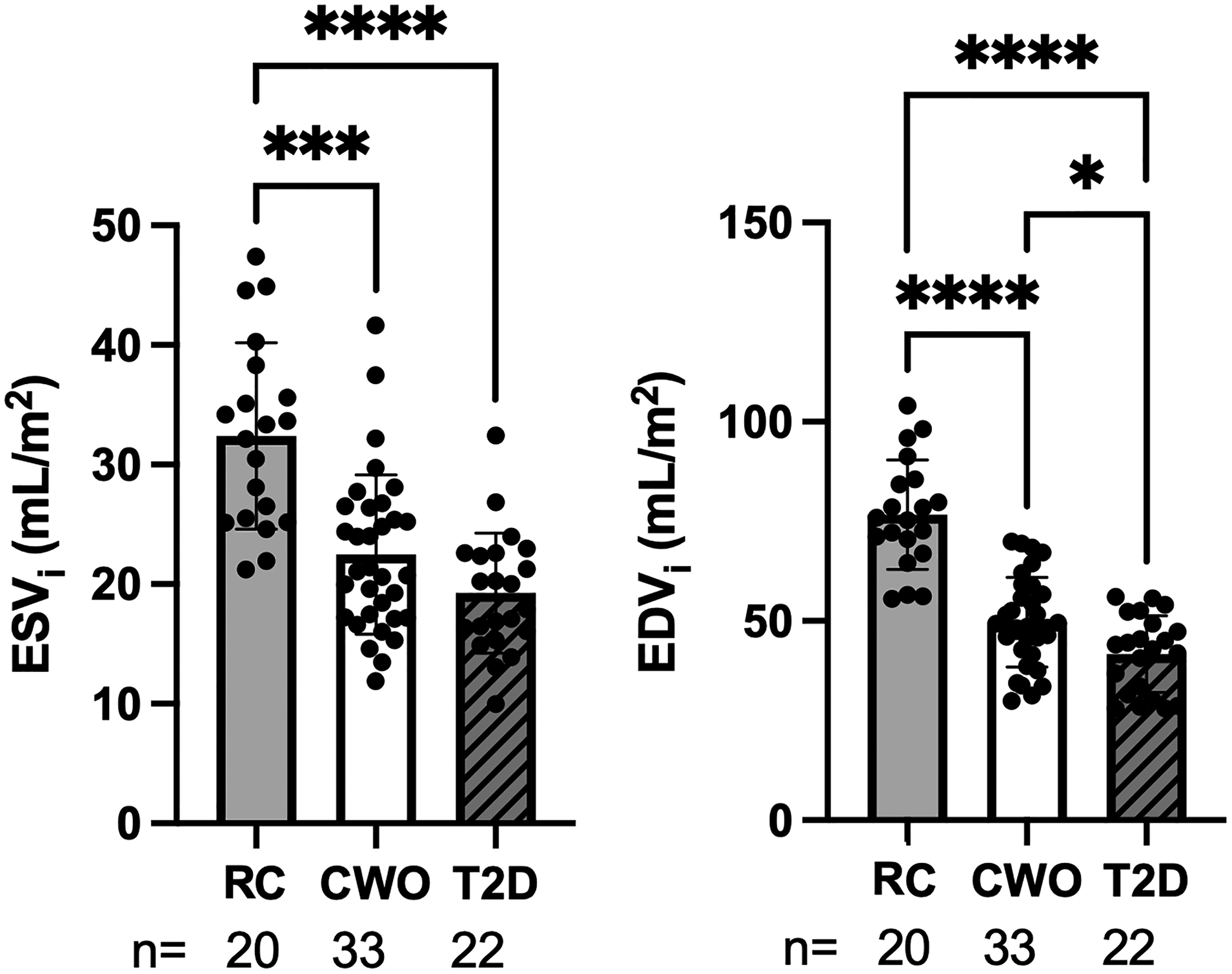
Results: Global arterial PWV did not differ between CWO and T2D. 2D PC-MRI PWV in the ascending aorta was higher in people with T2D compared with CWOs ( P < 0.01). 4D flow PWV in the thoracic aorta was higher in CWO ( P < 0.01), and T2D ( P < 0.001) compared with RC. End-diastolic volume, end-systolic volume, stroke volume, and cardiac output were lower in CWO and T2D groups compared with reference control.
Conclusion: Subclinical changes in arterial stiffening and cardiac remodeling in inactive CWO and T2D compared with reference control support obesity and/or physical inactivity as determinants of incipient CVD complications in uncomplicated T2D. Future studies should determine the mechanistic causes of the CVD complications in greater detail in order to create therapeutic targets.
Clinical trial registration: Cardiovascular Mechanisms of Exercise Intolerance in Diabetes and the Role of Sex (NCT03419195).
Copyright © 2023 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to declare. Research reported in this publication was supported, in part, by the National Institutes of Health’s National Institute on Aging, Grant Number P30AG059988 and K01AG080070. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Other funding includes the VA Clinical Merit CX001532 (JEBR), VA Merit BX002046, NIH-5T32HL007171, VA CDA2 BX004533 (RLS), NIH-NCATS, UL1TR001082 (JEBR, JGR, RLS), Ludeman Family Center for Women’s Health Research (RLS, JGR, JEBR, DE), ADA Cardiovascular Metabolism Fellowship Award 1-21-CMF-003 (LA), NIH pre-doctoral support T32DK120520 (DE), P30 DK116073 (JEBR), NIH/NCATS Colorado CTSA Grant Number KL2 TR002534 (EKE), AHA853697 (EKE), and ADA Junior Faculty Award 7-11-JF-42 (IES).
Figures
References
-
- Echouffo-Tcheugui JB, Xu H, DeVore AD, Schulte PJ, Butler J, Yancy CW, et al. Temporal trends and factors associated with diabetes mellitus among patients hospitalized with heart failure: Findings from Get With The Guidelines-Heart Failure registry. Am Heart J 2016; 182:9–20. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- P30 DK048520/DK/NIDDK NIH HHS/United States
- K12 AR084223/AR/NIAMS NIH HHS/United States
- K01 AG080070/AG/NIA NIH HHS/United States
- R56 DK088971/DK/NIDDK NIH HHS/United States
- KL2 TR002534/TR/NCATS NIH HHS/United States
- P30 DK116073/DK/NIDDK NIH HHS/United States
- P30 AG059988/AG/NIA NIH HHS/United States
- K24 HL145076/HL/NHLBI NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- K23 RR020038/RR/NCRR NIH HHS/United States
- T32 DK120520/DK/NIDDK NIH HHS/United States
- I01 CX001532/CX/CSRD VA/United States
- I01 BX002046/BX/BLRD VA/United States
- IK2 BX004533/BX/BLRD VA/United States
- T32 HL007171/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
