

Challenges in posterior uveitis-tips and tricks for the retina specialist
- PMID: 37589912
- PMCID: PMC10435440
- DOI: 10.1186/s12348-023-00342-5
Challenges in posterior uveitis-tips and tricks for the retina specialist
Abstract
Purpose: Posterior uveitis is a common chorioretinal pathology affecting all ages worldwide and is a frequent reason for referral to the retina clinic. The spectrum of etiologies for uveitis is very broad and includes infectious and auto-immune diseases. Inflammation can be confined to the eye or may be a part of systemic disease. A useful outline is therefore proposed to aid in the correct diagnosis of these challenging entities. The situation is further complicated by the fact that many neoplastic conditions resemble features of posterior uveitis; they are known as "masqueraders of uveitis". Here, we summarize different posterior uveitides that present with rare findings, along with masqueraders that can be difficult to distinguish. These conditions pose a diagnostic dilemma resulting in delay in treatment because of diagnostic uncertainty.
Methods: An extensive literature search was performed on the MEDLINE/PUBMED, EBSCO and Cochrane CENTRAL databases from January 1985 to January 2022 for original studies and reviews of predetermined diagnoses that include posterior uveitic entities, panuveitis and masquerade syndromes.
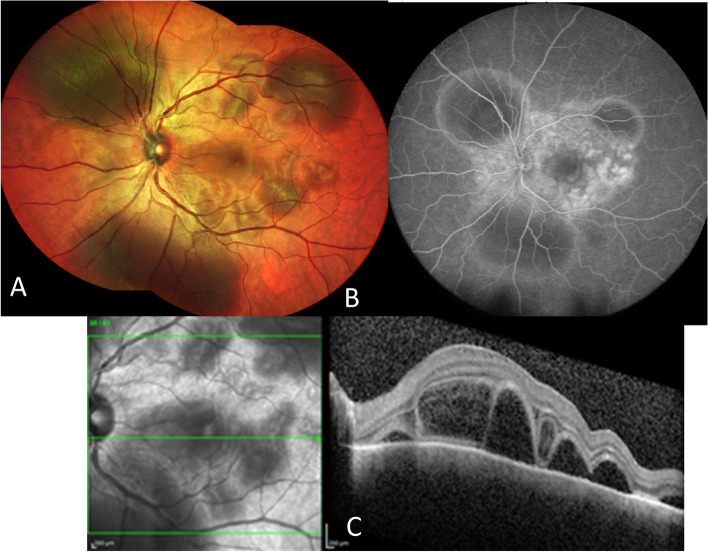
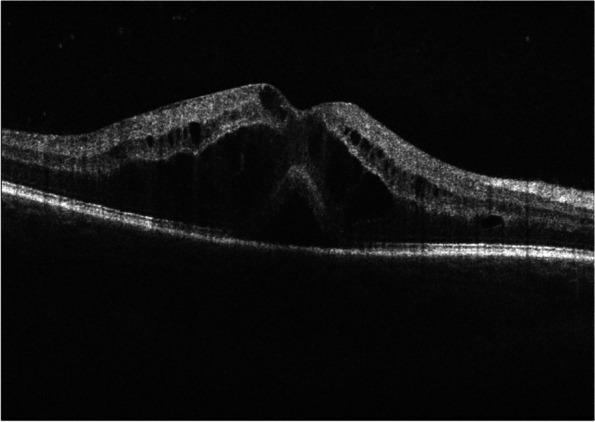
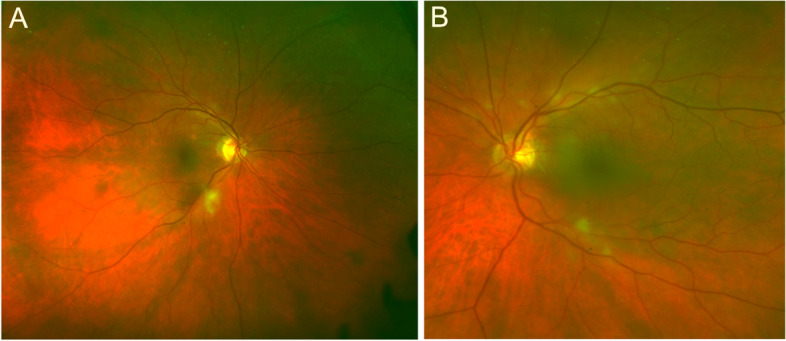
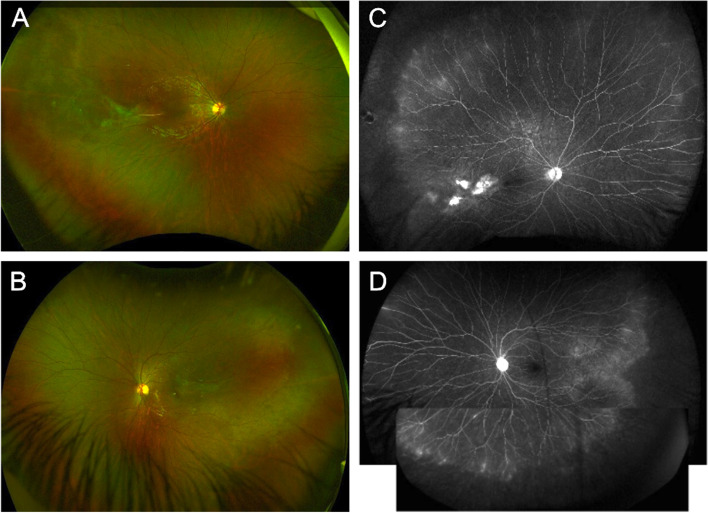
Results: We described conditions that can present as mimickers of posterior uveitis (i.e., immune check-points inhibitors and Vogt-Koyanagi-Harada-like uveitis; leukemia and lymphoma associated posterior uveitis), inflammatory conditions that present as mimickers of retinal diseases (i.e., Purtscher-like retinopathy as a presentation of systemic lupus erythematosus; central serous chorioretinopathy masquerading inflammatory exudative retinal detachment), and uveitic conditions with rare and diagnostically challenging etiologies (i.e., paradoxical inflammatory effects of anti-TNF-α; post vaccination uveitis; ocular inflammation after intravitreal injection of antiangiogenic drugs).
Conclusion: This review of unique posterior uveitis cases highlights the overlapping features of posterior uveitis (paradoxical inflammatory effects of anti -TNF α and uveitis; Purtscher-like retinopathy as a presentation of systemic lupus erythematosus, …) and the nature of retinal conditions (ischemic ocular syndrome, or central retinal vein occlusion, amyloidosis, inherited conditions like retinitis pigmentosa, autosomal dominant neovascular inflammatory vitreoretinopathy (ADNIV), etc.…) that may mimic them is represented. Careful review of past uveitis history, current medications and recent vaccinations, detailed examination of signs of past or present inflammation, eventually genetic testing and/ or multimodal retinal imaging (like fluorescein angiography, EDI-OCT, OCT-angiography for lupus Purtscher-like retinopathy evaluation, or ICG for central serous retinopathy, or retinal amyloid angiopathy) may aid in correct diagnosis.
Keywords: Birdshot choroidopathy; Check-point inhibitors retinopathy; MEK inhibitors retinopathy; Masquerades; Multifocal choroiditis uveitis; Ocular inflammation; Posterior uveitis; Punctate inner choroidopathy; Serpiginous choroiditis; Vogt- Koyanagi-Harada; White dot syndromes.
© 2023. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
