

Prophylactic anticoagulants for non-hospitalised people with COVID-19
- PMID: 37591523
- PMCID: PMC10428666
- DOI: 10.1002/14651858.CD015102.pub2
Prophylactic anticoagulants for non-hospitalised people with COVID-19
Abstract
Background: The coronavirus disease 2019 (COVID-19) pandemic has impacted healthcare systems worldwide. Multiple reports on thromboembolic complications related to COVID-19 have been published, and researchers have described that people with COVID-19 are at high risk for developing venous thromboembolism (VTE). Anticoagulants have been used as pharmacological interventions to prevent arterial and venous thrombosis, and their use in the outpatient setting could potentially reduce the prevalence of vascular thrombosis and associated mortality in people with COVID-19. However, even lower doses used for a prophylactic purpose may result in adverse events such as bleeding. It is important to consider the evidence for anticoagulant use in non-hospitalised people with COVID-19.
Objectives: To evaluate the benefits and harms of prophylactic anticoagulants versus active comparators, placebo or no intervention, or non-pharmacological interventions in non-hospitalised people with COVID-19.
Search methods: We used standard, extensive Cochrane search methods. The latest search date was 18 April 2022.
Selection criteria: We included randomised controlled trials (RCTs) comparing prophylactic anticoagulants with placebo or no treatment, another active comparator, or non-pharmacological interventions in non-hospitalised people with COVID-19. We included studies that compared anticoagulants with a different dose of the same anticoagulant. We excluded studies with a duration of under two weeks.
Data collection and analysis: We used standard Cochrane methodological procedures. Our primary outcomes were all-cause mortality, VTE (deep vein thrombosis (DVT) or pulmonary embolism (PE)), and major bleeding. Our secondary outcomes were DVT, PE, need for hospitalisation, minor bleeding, adverse events, and quality of life. We used GRADE to assess the certainty of the evidence.
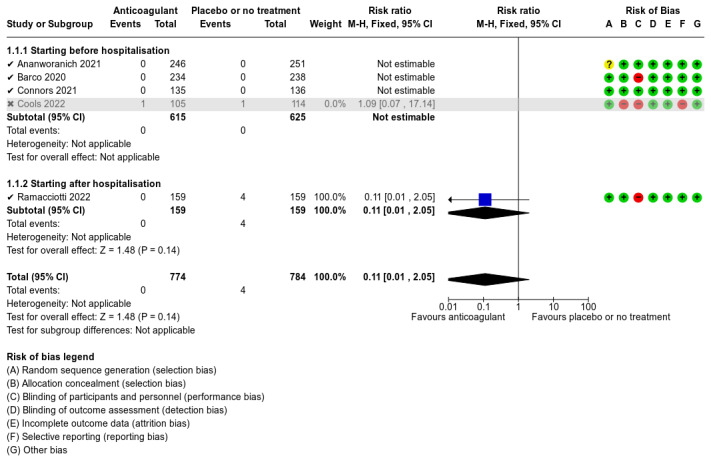
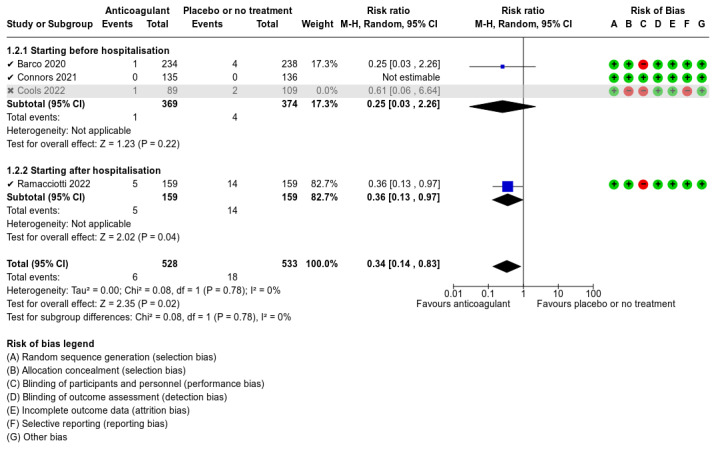
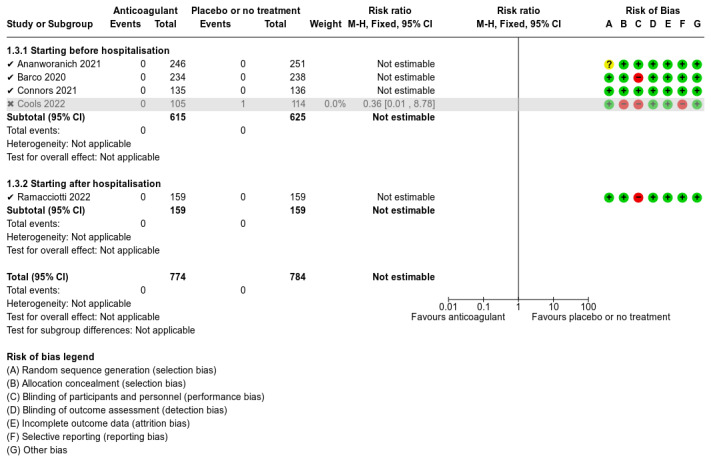
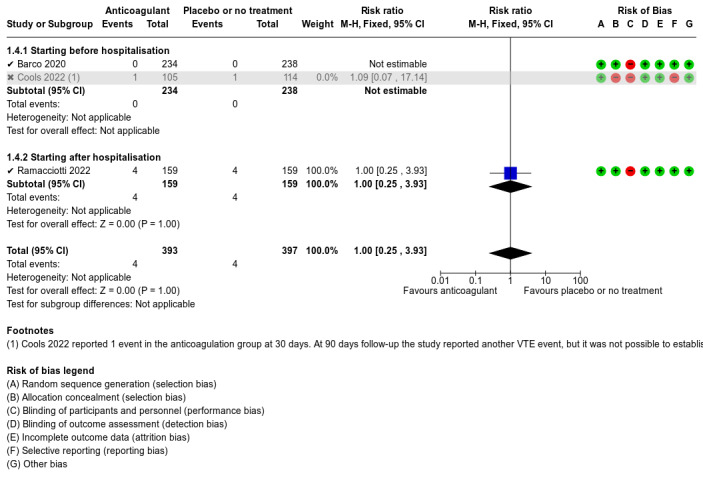
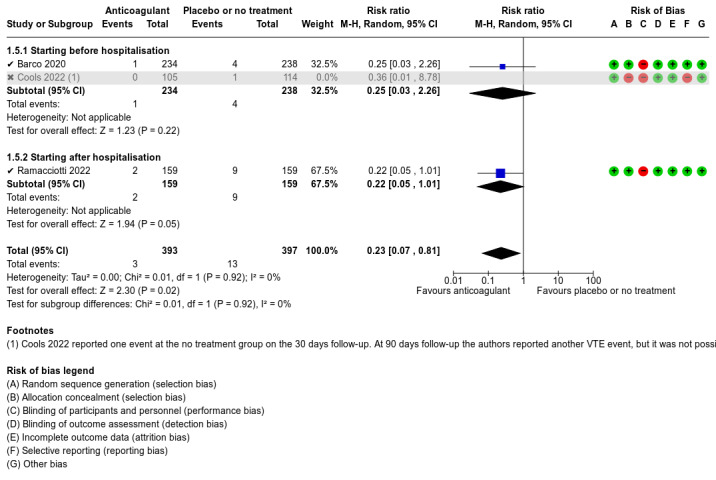
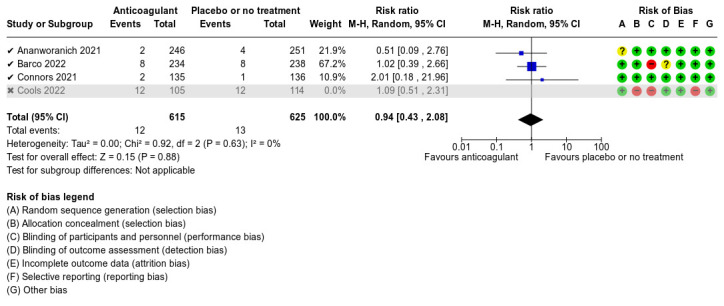
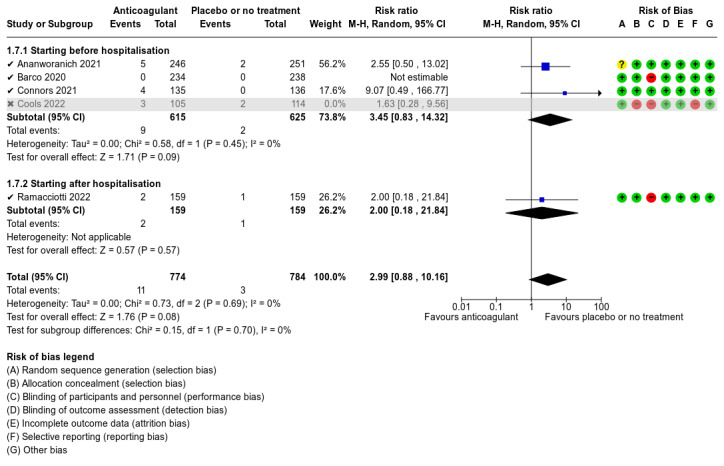
Main results: We included five RCTs with up to 90 days of follow-up (short term). Data were available for meta-analysis from 1777 participants. Anticoagulant compared to placebo or no treatment Five studies compared anticoagulants with placebo or no treatment and provided data for three of our outcomes of interest (all-cause mortality, major bleeding, and adverse events). The evidence suggests that prophylactic anticoagulants may lead to little or no difference in all-cause mortality (risk ratio (RR) 0.36, 95% confidence interval (CI) 0.04 to 3.61; 5 studies; 1777 participants; low-certainty evidence) and probably reduce VTE from 3% in the placebo group to 1% in the anticoagulant group (RR 0.36, 95% CI 0.16 to 0.85; 4 studies; 1259 participants; number needed to treat for an additional beneficial outcome (NNTB) = 50; moderate-certainty evidence). There may be little to no difference in major bleeding (RR 0.36, 95% CI 0.01 to 8.78; 5 studies; 1777 participants; low-certainty evidence). Anticoagulants probably result in little or no difference in DVT (RR 1.02, 95% CI 0.30 to 3.46; 3 studies; 1009 participants; moderate-certainty evidence), but probably reduce the risk of PE from 2.7% in the placebo group to 0.7% in the anticoagulant group (RR 0.25, 95% CI 0.08 to 0.79; 3 studies; 1009 participants; NNTB 50; moderate-certainty evidence). Anticoagulants probably lead to little or no difference in reducing hospitalisation (RR 1.01, 95% CI 0.59 to 1.75; 4 studies; 1459 participants; moderate-certainty evidence) and may lead to little or no difference in adverse events (minor bleeding, RR 2.46, 95% CI 0.90 to 6.72; 5 studies, 1777 participants; low-certainty evidence). Anticoagulant compared to a different dose of the same anticoagulant One study compared anticoagulant (higher-dose apixaban) with a different (standard) dose of the same anticoagulant and reported five relevant outcomes. No cases of all-cause mortality, VTE, or major bleeding occurred in either group during the 45-day follow-up (moderate-certainty evidence). Higher-dose apixaban compared to standard-dose apixaban may lead to little or no difference in reducing the need for hospitalisation (RR 1.89, 95% CI 0.17 to 20.58; 1 study; 278 participants; low-certainty evidence) or in the number of adverse events (minor bleeding, RR 0.47, 95% CI 0.09 to 2.54; 1 study; 278 participants; low-certainty evidence). Anticoagulant compared to antiplatelet agent One study compared anticoagulant (apixaban) with antiplatelet agent (aspirin) and reported five relevant outcomes. No cases of all-cause mortality or major bleeding occurred during the 45-day follow-up (moderate-certainty evidence). Apixaban may lead to little or no difference in VTE (RR 0.36, 95% CI 0.01 to 8.65; 1 study; 279 participants; low-certainty evidence), need for hospitalisation (RR 3.20, 95% CI 0.13 to 77.85; 1 study; 279 participants; low-certainty evidence), or adverse events (minor bleeding, RR 2.13, 95% CI 0.40 to 11.46; 1 study; 279 participants; low-certainty evidence). No included studies reported on quality of life or investigated anticoagulants compared to a different anticoagulant, or anticoagulants compared to non-pharmacological interventions.
Authors' conclusions: We found low- to moderate-certainty evidence from five RCTs that prophylactic anticoagulants result in little or no difference in major bleeding, DVT, need for hospitalisation, or adverse events when compared with placebo or no treatment in non-hospitalised people with COVID-19. Low-certainty evidence indicates that prophylactic anticoagulants may result in little or no difference in all-cause mortality when compared with placebo or no treatment, but moderate-certainty evidence indicates that prophylactic anticoagulants probably reduce the incidence of VTE and PE. Low-certainty evidence suggests that comparing different doses of the same prophylactic anticoagulant may result in little or no difference in need for hospitalisation or adverse events. Prophylactic anticoagulants may result in little or no difference in risk of VTE, hospitalisation, or adverse events when compared with antiplatelet agents (low-certainty evidence). Given that there were only short-term data from one study, these results should be interpreted with caution. Additional trials of sufficient duration are needed to clearly determine any effect on clinical outcomes.
پیشینه: پاندمی یا همهگیری بیماری کروناویروس 2019 (COVID‐19) سیستمهای مراقبتهای سلامت را در سراسر جهان تحت تاثیر قرار داده است. گزارشهای متعددی در مورد عوارض ترومبوآمبولی مرتبط با کووید‐19 منتشر شده، و محققان توضیح دادهاند که افراد مبتلا به کووید‐19 در معرض خطر بالای ابتلا به ترومبوآمبولی وریدی (venous thromboembolism; VTE) قرار دارند. آنتیکوآگولانتها (anticoagulant) به عنوان مداخلات دارویی برای پیشگیری از وقوع ترومبوز شریانی و وریدی مورد استفاده قرار گرفتهاند، و استفاده از آنها در شرایط سرپایی میتواند بهطور بالقوه شیوع ترومبوز عروقی و مورتالیتی مرتبط با آن را در افراد مبتلا به کووید‐19 کاهش دهد. با این حال، حتی دوزهای پائینتر که برای اهداف پروفیلاکتیک استفاده میشوند ممکن است منجر به بروز عوارض جانبی مانند خونریزی شوند. در نظر گرفتن شواهدی مبنی بر استفاده از آنتیکوآگولانتها در افراد غیر بستری مبتلا به کووید‐19 اهمیت زیادی دارد. اهداف: ارزیابی فواید و مضرات آنتیکوآگولانتهای پروفیلاکتیک در مقابل گروههای مقایسه فعال، دارونما (placebo) یا عدم مداخله، یا مداخلات غیر دارویی در افراد غیر بستری مبتلا به کووید‐19. روشهای جستوجو: از روشهای استاندارد و جامع جستوجوی کاکرین استفاده کردیم. تاریخ آخرین جستوجو، 18 اپریل 2022 بود. معیارهای انتخاب: کارآزماییهای تصادفیسازی و کنترل شدهای (randomised controlled trials; RCTs) را وارد کردیم که آنتیکوآگولانتهای پروفیلاکتیک را با دارونما یا عدم درمان، مقایسهکننده فعال دیگر، یا مداخلات غیر دارویی در افراد غیر بستری مبتلا به کووید‐19 مقایسه کردند. مطالعاتی را وارد کردیم که آنتیکوآگولانتها را با دوز متفاوتی از همان آنتیکوآگولانت مقایسه کردند. مطالعاتی را با طول دوره کمتر از دو هفته حذف کردیم. گردآوری و تجزیهوتحلیل دادهها: از پروسیجرهای استاندارد روششناسی (methodology) کاکرین استفاده کردیم. پیامدهای اولیه عبارت بودند از مورتالیتی به هر علتی (all‐cause mortality)، VTE (ترومبوز ورید عمقی ((deep vein thrombosis; DVT) یا آمبولی ریه (pulmonary embolism; PE))، و خونریزی شدید. پیامدهای ثانویه، شامل DVT؛ PE، نیاز به بستری در بیمارستان، خونریزی خفیف، عوارض جانبی، و کیفیت زندگی بودند. برای ارزیابی قطعیت شواهد از سیستم درجهبندی توصیه، ارزیابی، توسعه و ارزشیابی (Grading of Recommendations Assessment, Development and Evaluation; GRADE) استفاده کردیم. نتایج اصلی: پنج RCT را با حداکثر 90 روز دوره پیگیری (کوتاهمدت) وارد کردیم. دادههای 1777 شرکتکننده برای متاآنالیز موجود بودند. مصرف آنتیکوآگولانت در مقایسه با دارونما یا عدم درمان پنج مطالعه آنتیکوآگولانتها را با دارونما یا عدم درمان مقایسه کرده و دادههایی را برای سه مورد از پیامدهای مورد نظر (مورتالیتی به هر علتی، خونریزی شدید، و عوارض جانبی) ارائه دادند. شواهد نشان میدهد که آنتیکوآگولانتهای پروفیلاکتیک ممکن است منجر به تفاوتی اندک یا عدم تفاوت در مورتالیتی به هر علتی شده (خطر نسبی (RR): 0.36؛ 95% فاصله اطمینان (CI): 0.04 تا 3.61؛ 5 مطالعه؛ 1777 شرکتکننده؛ شواهد با قطعیت پائین) و احتمالا VTE از 3% در گروه دارونما به 1% در گروه آنتیکوآگولانتها برسانند (RR: 0.36؛ 95% CI؛ 0.16 تا 0.85؛ 4 مطالعه؛ 1259 شرکتکننده؛ تعداد افراد مورد نیاز جهت درمان تا حصول یک پیامد مفید بیشتر (number needed to treat for an additional beneficial outcome; NNTB): 50؛ شواهد با قطعیت متوسط). ممکن است تفاوتی اندک تا عدم تفاوت در خونریزی شدید وجود داشته باشد (RR: 0.36؛ 95% CI؛ 0.01 تا 8.78؛ 5 مطالعه؛ 1777 شرکتکننده؛ شواهد با قطعیت پائین). آنتیکوآگولانتها احتمالا منجر به تفاوتی اندک یا عدم تفاوت در DVT میشوند (RR: 1.02؛ 95% CI؛ 0.30 تا 3.46؛ 3 مطالعه؛ 1009 شرکتکننده؛ شواهد با قطعیت متوسط)، اما احتمالا خطر PE را از 2.7% در گروه دارونما به 0.7% در گروه آنتیکوآگولانتها کاهش میدهند (RR: 0.25؛ 95% CI؛ 0.08 تا 0.79؛ 3 مطالعه؛ 1009 شرکتکننده؛ NNTB: 50؛ شواهد با قطعیت متوسط). آنتیکوآگولانتها احتمالا منجر به تفاوتی اندک یا عدم تفاوت در کاهش بستری شدن در بیمارستان شده (RR: 1.01؛ 95% CI؛ 0.59 تا 1.75؛ 4 مطالعه؛ 1459 شرکتکننده؛ شواهد با قطعیت متوسط) و ممکن است منجر به تفاوتی اندک یا عدم تفاوت در بروز عوارض جانبی شوند (خونریزی خفیف، RR: 2.46؛ 95% CI؛ 0.90 تا 6.72؛ 5 مطالعه، 1777 شرکتکننده؛ شواهد با قطعیت پائین). مصرف آنتیکوآگولانت در مقایسه با دوز متفاوتی از همان آنتیکوآگولانت یک مطالعه آنتیکوآگولانت (آپیکسابان (apixaban) با دوز بالاتر) را با دوز متفاوتی (استاندارد) از همان آنتیکوآگولانت مقایسه کرده و پنج پیامد مرتبط را گزارش کرد. هیچ موردی از مورتالیتی به هر علتی، VTE، یا خونریزی شدید در هر دو گروه در طول دوره پیگیری 45 روز رخ نداد (شواهد با قطعیت متوسط). آپیکسابان با دوز بالاتر در مقایسه با آپیکسابان با دوز استاندارد ممکن است منجر به تفاوتی اندک یا عدم تفاوت در کاهش نیاز به بستری شدن در بیمارستان (RR: 1.89؛ 95% CI؛ 0.17 تا 20.58؛ 1 مطالعه؛ 278 شرکتکننده؛ شواهد با قطعیت پائین) یا در تعداد عوارض جانبی (خونریزی خفیف، RR: 0.47؛ 95% CI؛ 0.09 تا 2.54؛ 1 مطالعه؛ 278 شرکتکننده؛ شواهد با قطعیت پائین) شود. مصرف آنتیکوآگولانت در مقایسه با عامل ضد پلاکت یک مطالعه آنتیکوآگولانت (آپیکسابان) را با عامل ضد پلاکت (آسپرین) مقایسه کرده و پنج پیامد مرتبط را گزارش کرد. هیچ موردی از مورتالیتی به هر علتی یا خونریزی شدید در طول دوره پیگیری 45 روز رخ نداد (شواهد با قطعیت متوسط). آپیکسابان ممکن است منجر به تفاوتی اندک یا عدم تفاوت در VTE (RR: 0.36؛ 95% CI؛ 0.01 تا 8.65؛ 1 مطالعه؛ 279 شرکتکننده؛ شواهد با قطعیت پائین)، نیاز به بستری شدن (RR: 3.20؛ 95% CI؛ 0.13 تا 77.85؛ 1 مطالعه؛ 279 شرکتکننده؛ شواهد با قطعیت پائین)، یا عوارض جانبی (خونریزی خفیف، RR: 2.13؛ 95% CI؛ 0.40 تا 11.46؛ 1 مطالعه؛ 279 شرکتکننده؛ شواهد با قطعیت پائین) شود. هیچ یک از مطالعات وارد شده کیفیت زندگی را گزارش نکرده یا آنتیکوآگولانت را در مقایسه با یک آنتیکوآگولانت متفاوت، یا آنتیکوآگولانت را در مقایسه با مداخلات غیر دارویی بررسی نکردند. نتیجهگیریهای نویسندگان: شواهدی را با قطعیت پائین تا متوسط از پنج RCT به دست آوردیم که آنتیکوآگولانتهای پروفیلاکتیک در مقایسه با دارونما یا عدم درمان در افراد غیر بستری مبتلا به کووید‐19، باعث تفاوتی اندک یا عدم تفاوت در بروز خونریزی شدید، DVT، نیاز به بستری در بیمارستان، یا عوارض جانبی میشوند. شواهدی با قطعیت پائین نشان میدهد که آنتیکوآگولانتهای پروفیلاکتیک در مقایسه با دارونما یا عدم درمان، ممکن است منجر به تفاوتی اندک یا عدم تفاوت در مورتالیتی به هر علتی شوند، اما شواهدی با قطعیت متوسط نشان میدهد که آنتیکوآگولانتهای پروفیلاکتیک احتمالا بروز VTE و PE را کاهش میدهند. شواهدی با قطعیت پائین حاکی از آن است که مقایسه دوزهای مختلف از یک آنتیکوآگولانت پروفیلاکتیک ممکن است منجر به تفاوتی اندک یا عدم تفاوت در نیاز به بستری شدن در بیمارستان یا بروز عوارض جانبی شود. آنتیکوآگولانتهای پروفیلاکتیک در مقایسه با عوامل ضد پلاکت ممکن است تفاوتی اندک یا عدم تفاوت را در خطر ابتلا به VTE، بستری شدن در بیمارستان، یا ابتلا به عوارض جانبی ایجاد کنند (شواهد با قطعیت پائین). با توجه به اینکه دادههای کوتاهمدت فقط از یک مطالعه به دست آمدند، این نتایج باید با احتیاط تفسیر شوند. انجام کارآزماییهای بیشتر با طول دوره کافی برای تعیین هر تاثیری از مداخله بر پیامدهای بالینی مورد نیاز است.
Trial registration: ClinicalTrials.gov NCT04504032 NCT04400799 NCT04498273 NCT04492254 NCT04662684 NCT04401293 NCT04508023 NCT04542408 NCT04650087 NCT04715295 NCT04746339 NCT04757857 NCT04508439.
Copyright © 2023 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
BCS: none known; BCS has declared that she works as a private practice vascular surgeon, dealing with both venous and arterial diseases. RLGF: none known; RLGF has declared he is professor of vascular surgery at Universidade Federal de São Paulo, Brazil. VTC: none known ANA: none known; ANA has declared he is director of Cochrane Brazil. LCUN: none known
Figures

























Update of
References
References to studies included in this review
Ananworanich 2021 {published data only (unpublished sought but not used)}
-
- Ananworanich J, Mogg R, Dunne MW, Bassyouni M, David CV, Gonzalez E, et al. Randomized study of rivaroxaban vs placebo on disease progression and symptoms resolution in high-risk adults with mild COVID-19. Clinical Infectious Diseases 2021;75(1):e473-e481. [DOI: 10.1093/cid/ciab813] - DOI - PMC - PubMed
-
- NCT04504032. A trial to evaluate safety and efficacy of rivaroxaban (COVID-19). clinicaltrials.gov/ct2/show/NCT04504032 2020. [CLINICALTRIALS.GOV: NCT04504032]
Barco 2022 {published data only (unpublished sought but not used)}
-
- Barco S, Bingisser R, Colucci G, Frenk A, Gerber B, Held U, et al. Enoxaparin for primary thromboprophylaxis in ambulatory patients with coronavirus disease-2019 (the OVID study): a structured summary of a study protocol for a randomized controlled trial. Trials 2020;21(1):770. [DOI: 10.1186/s13063-020-04678-4] - DOI - PMC - PubMed
-
- Barco S, Voci D, Bingisser R, Colucci G, Frenk A, Gerber B, et al. Enoxaparin for primary thromboprophylaxis in ambulatory patients with COVID-19: the multicentre randomized controlled investigatorinitiated OVID trial. Study design, status or enrolment and patients overview. Vasa - European Journal of Vascular Medicine 2021;50(Suppl 107):15.
-
- Barco S, Voci D, Bingisser R, Colucci G, Frenk A, Gerber B, et al. Enoxaparin for primary thromboprophylaxis in ambulatory patients with COVID-19: the multicentre randomized controlled investigatorinitiated OVID trial. Study design, status or enrolment and patients overview. Vasa - European Journal of Vascular Medicine 2021;50(Suppl 107):15. [DOI: 10.1024/0301-1526/a000973] - DOI
Connors 2021 {published data only}
-
- Connors JM, Brooks MM, Sciurba FC, Krishnan JA, Bledsoe JR, Kindzelski A, et al. Effect of antithrombotic therapy on clinical outcomes in outpatients with clinically stable symptomatic COVID-19: the ACTIV-4B randomized clinical trial. JAMA 2021;326(17):1703-12. [DOI: 10.1001/jama.2021.17272] - DOI - PMC - PubMed
-
- Hulbert JC, Krishnan JA, Heather E, Shapiro N, O'Neal S, Baucom A, et al. A novel approach to medical monitoring during the SARS-CoV-2 pandemic supporting the ACTIV 4B outpatient anticoagulation trial. American Journal of Respiratory and Critical Care Medicine 2021;203:A1749. [DOI: ]
Cools 2022 {published data only}
-
- Cools F, Virdone S, Sawhney J, Lopes R, Jacobson B, Arcelus J, ETHIC investigators, et al. Thromboprophylactic low-molecular-weight heparin versus standard of care in unvaccinated, at-risk outpatients with COVID-19 (ETHIC): an open-label, multicentre, randomised, controlled, phase 3b trial. Lancet Haematology 2022;9(8):e594-e604. [DOI: 10.1016/S2352-3026(22)00173-9] - DOI - PMC - PubMed
-
- NCT04492254. ETHIC trial: early LMWH in symptomatic COVID-19 positive patients. clinicaltrials.gov/ct2/show/NCT04492254 2020. [NCT04492254]
Ramacciotti 2022 {published data only}
-
- NCT04662684. Medically ill hospitalized patients for COVID-19 thrombosis extended prophylaxis with rivaroxaban therapy: the MICHELLE trial (MICHELLE). clinicaltrials.gov/ct2/show/NCT04662684 2020. [CLINICALTRIALS.GOV: NCT04662684]
-
- Ramacciotti E, Agati LB, Calderaro D, Volpiani GG, Oliveira CC, Aguiar VCR, et al. Medically ill hospitalized patients for COVID-19 thrombosis extended prophylaxis with rivaroxaban therapy: rationale and design of the MICHELLE trial. American Heart Journal 2021;242:115-22. [DOI: 10.1016/j.ahj.2021.08.016] - DOI - PMC - PubMed
-
- Ramacciotti E, Barile Agati L, Calderaro D, Aguiar VC, Spyropoulos AC, Oliveira CC, Michelle investigators, et al. Rivaroxaban versus no anticoagulation for post-discharge thromboprophylaxis after hospitalisation for COVID-19 (MICHELLE): an open-label, multicentre, randomised, controlled trial. Lancet 2022;399(10319):50-9. [DOI: ] - PMC - PubMed
References to studies excluded from this review
Aghamohammadi 2020 {published data only}
Borghi 2021 {published data only}
-
- Borghi B, Borghi R, Deamicis T, Sommariva C, Pipino G. Early use of fondaparinux at therapeutic dosage in COVID-19 infection. Minerva Anestesiologica 2021;87(8):958-60. - PubMed
ChiCTR2000034796 {published data only}ChiCTR2000034796
-
- ChiCTR2000034796. The efficacy and safety of heparin in the treatment of novel coronavirus pneumonia (COVID-19): a retrospective single center clinical trial. https://trialsearch.who.int/Trial2.aspx?TrialID=ChiCTR2000034796 2020.
JPRN‐UMIN000042489 {published data only}JPRN‐UMIN000042489
-
- JPRN-UMIN000042489. Antiinflammatory and anticoagulative agents in COVID-19 pneumonia treatment. who.int/trialsearch/Trial2.aspx?TrialID=JPRN-UMIN000042489 2020.
Kuno 2022 {published data only}
Lisker 2021 {published data only}
-
- Lisker G, Narasimhan M, Greenberg H, Ramdeo R, McGinn T. Ambulatory management of moderate to high risk COVID-19 patients: the coronavirus related outpatient work navigators (CROWN) protocol. Home Health Care Management and Practice 2021;33(1):49-53. [DOI: 10.1177/1084822320964196] - DOI
Rivera‐Caravaca 2021 {published data only}
-
- Rivera-Caravaca JM, Buckley BJ, Harrison SL, Fazio-Eynullayeva E, Underhill P, Marin F, et al. Direct-acting oral anticoagulants use prior to COVID-19 diagnosis and associations with 30-day clinical outcomes. Thrombosis Research 2021;205:1-7. [DOI: 10.1016/j.thromres.2021.06.014] - DOI - PMC - PubMed
Sharma 2021 {published data only}
-
- Sharma A, Sharma C, Raina S, Singh B, Dadhwal D, Dogra V, et al. A randomized open-label trial to evaluate the efficacy and safety of triple therapy with aspirin, atorvastatin, and nicorandil in hospitalised patients with SARS Cov-2 infection: a structured summary of a study protocol for a randomized controlled trial. Trials Journal 2021;22:451. [DOI: 10.1186/s13063-021-05361-y] - DOI - PMC - PubMed
Spyropoulos 2021 {published data only}
-
- Goldin M, Giannis D, Diab W, Wang J, Khanijo S, Sharifova G, et al. Treatment-dose LMWH versus prophylactic/intermediate dose heparins in high-risk COVID-19 inpatients: rationale and design of the HEP-COVID trial. Thrombosis and Haemostasis 2021;121(12):1684-95. [DOI: 10.1055/a-1475-2351] - DOI - PubMed
-
- Spyropoulos AC, Goldin M, Dimitrios G. Efficacy and safety of therapeutic-dose heparin vs standard prophylactic or intermediate-dose heparins for thromboprophylaxis in high-risk hospitalized patients with COVID-19. The HEP-COVID randomized clinical trial. Heart International 2021;15(2):62-4. [PMID: 10.1001/jamainternmed.2021.6203] - DOI - PMC - PubMed
Vergori 2021 {published data only}
References to ongoing studies
Capell 2021 {published data only}
-
- Capell WH, Barnathan ES, Piazza G, Spyropoulos AC, Hsia J, Bull S, et al. Rationale and design for the study of rivaroxaban to reduce thrombotic events, hospitalization and death in outpatients with COVID-19: the PREVENT-HD study. American Heart Journal 2021;235:12-23. [DOI: 10.1016/j.ahj.2021.02.001] - DOI - PMC - PubMed
-
- NCT04508023. A study of rivaroxaban to reduce the risk of major venous and arterial thrombotic events, hospitalization and death in medically ill outpatients with acute, symptomatic coronavirus disease 2019 (COVID-19) infection (PREVENT-HD). clinicaltrials.gov/ct2/show/NCT04508023 (first received 11 August 2020). [CLINICALTRIALS.GOV: NCT04508023]
EUCTR2020‐005884‐29‐IT {published data only}EUCTR2020‐005884‐29‐IT
-
- EUCTR2020-005884-29-IT. Role of heparin in the prevention of thromboembolism in patients with COVID-19 and respiratory failure. trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2020-005884-29-IT (first received 8 June 2021).
NCT04542408 {published data only}
-
- NCT04542408. Hamburg edoxaban for anticoagulation in COVID-19 Study. clinicaltrials.gov/show/NCT04542408 (first received 9 September 2020). [CLINICALTRIALS.GOV: NCT04542408]
NCT04650087 {published data only}
-
- NCT04650087. COVID-19 thrombosis prevention trials: post-hospital thromboprophylaxis. clinicaltrials.gov/ct2/show/NCT04650087 (first received 2 December 2020). [CLINICALTRIALS.GOV: NCT04650087]
NCT04715295 {published data only}
-
- NCT04715295. Safety and Efficacy of Doxycycline and Rivaroxaban in COVID-19. clinicaltrials.gov/show/NCT04715295 (first received 20 January 2021).
NCT04746339 {published data only}
-
- NCT04746339. Apixaban for prophylaxis of thromboembolic outcomes in COVID-19. clinicaltrials.gov/show/NCT04746339 (first received 9 February 2021). [CLINICALTRIALS.GOV: NCT04746339]
NCT04757857 {published data only}
-
- NCT04757857. COVID-19 antithrombotic rivaroxaban evaluation. clinicaltrials.gov/ct2/show/NCT04757857 (first received 17 February 2021). [CLINICALTRIALS.GOV: NCT04757857]
Ramos‐Peñafiel 2020 {published data only}
-
- NCT04508439. Effect of the use of anticoagulant therapy during hospitalization and discharge in patients with COVID-19 infection. clinicaltrials.gov/show/NCT04508439 (first received 11 August 2020). [CLINICALTRIALS.GOV: NCT04508439]
-
- Ramos C, Madera E, Majlufc A, Cabrera A, MacEdo D, Valencia U, et al. Effect of rivaroxaban (10mg) versus observation on the risk of thrombosis at discharge in individuals with covid-19. HemaSphere 2021;5(Suppl 2):645. [EMBASE: covidwho-1393448]
RBR‐7nzwkpg {published data only}RBR‐7nzwkpg
-
- RBRnzwkpg. Effects of treatment with oral anticoagulant associated with antibiotics on clinical, immunological, hospitalization and death parameters in patients with suspected Covid-19 infection and coagulation disorders. trialsearch.who.int/Trial2.aspx?TrialID=RBR-7nzwkpg (first received 6 January 2021).
Additional references
Acosta 2008
-
- Acosta S, Alhadad A, Svensson P, Ekberg O. Epidemiology, risk and prognostic factors in mesenteric venous thrombosis. British Journal of Surgery 2008;95(10):1245-51. [PMID: ] - PubMed
Alikhan 2014
Amaral 2022
Anderson 2003
-
- Anderson FA, Spencer FA. Risk factors for venous thromboembolism. Circulation 2003;107(23 (suppl 1)):I-9. - PubMed
Atkins 2004
Barbar 2010
-
- Barbar S, Noventa F, Rossetto V, Ferrari A, Brandolin B, Perlati M, et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction Score. Journal of Thrombosis and Haemostasis 2010;8(11):2450-7. [PMID: ] - PubMed
Barco 2020
-
- Barco S, Bingisser R, Colucci G, Frenk A, Gerber B, Held U, et al. Enoxaparin for primary thromboprophylaxis in ambulatory patients with coronavirus disease-2019 (the OVID study): a structured summary of a study protocol for a randomized controlled trial. Trials 2020;21(1):770. [PMID: ] - PMC - PubMed
Bautista‐Vargas 2020
Benson 2021
Benzakoun 2020
Biagioni 2020
-
- Biagioni RB, Lopes RD, Agati LB, Sacilotto R, Wolosker N, Sobreira ML, et al. Rationale and design for the study apixaban versus clopidogrel on a background of aspirin in patient undergoing infrapopliteal angioplasty for critical limb ischemia: AGRIPPA trial. American Heart Journal 2020;227:100-6. [PMID: ] - PubMed
Bikdeli 2020
Broderick 2021
Capell 2021
Cogo 1993
-
- Cogo A, Lensing AW, Prandoni P, Hirsh J. Distribution of thrombosis in patients with symptomatic deep vein thrombosis. Implications for simplifying the diagnostic process with compression ultrasound. Archives of Internal Medicine 1993;153(24):2777-80. [PMID: ] - PubMed
COMET 2021
-
- Core outcome set developers’ response to COVID-19 (April 2021). comet-initiative.org/Studies/Details/1538 (accessed 25 May 2021).
Correia 2022
COVER 2022
COVIDSurg 2021a
COVIDSurg 2021b
COVIDSurg 2022a
COVIDSurg 2022b
Cuker 2021
Deeks 2021
-
- Deeks JJ, Higgins JP, Altman DG, editor(s). Chapter 10: Analysing data and undertaking meta-analyses. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page M, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook/archive/v6.2.
Emert 2020
Fernandes 2019
Flumignan 2015
Flumignan 2021
Flumignan 2022a
Flumignan 2022b
Flumignan 2023
Giannis 2021
Goshua 2020
GRADEpro GDT [Computer program]
-
- GRADEpro GDT. Version accessed 15 March 2022. Hamilton (ON): McMaster University (developed by Evidence Prime). Available from gradepro.org.
Graphreader 2022
-
- Larsen K. Graphreader. www.graphreader.com/ (accessed 10 April 2022).
Guyatt 2012
-
- Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schünemann HJ, American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis Panel. Executive summary: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012;141((2 Suppl)):7S-47S. [DOI: 10.1378/chest.1412S3] - DOI - PMC - PubMed
Handoll 2015
Hanff 2020
Higgins 2017
-
- Higgins JP, Altman DG, Sterne JA, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s), Cochrane Handbook for Systematic Reviews of Interventions Version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook/archive/v5.2.
Higgins 2021
-
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook/archive/v6.2.
Hippensteel 2020
Hirsh 1986
-
- Hirsh J, Hull RD, Raskob GE. Clinical features and diagnosis of venous thrombosis. Journal of the American College of Cardiology 1986;8(6 (suppl B)):114B-27B. [PMID: ] - PubMed
Kahn 2014
Kakkos 2021
-
- Kakkos SK, Gohel M, Baekgaard N, Bauersachs R, Bellmunt-Montoya S, Black SA, et al. Editor's Choice - European Society for Vascular Surgery (ESVS) 2021 Clinical Practice Guidelines on the Management of Venous Thrombosis. European Journal of Vascular and Endovascular Surgery 2021;61(1):9-82. [PMID: ] - PubMed
Kakkos 2022
-
- Kakkos S, Kirkilesis G, Caprini JA, Geroulakos G, Nicolaides A, Stansby G, et al. Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism. Cochrane Database of Systematic Reviews 2022, Issue 1. Art. No: CD005258. [DOI: 10.1002/14651858.CD005258.pub4] - DOI - PMC - PubMed
Kearon 2016
-
- Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 2016;149(2):315-52. - PubMed
Kelliher 2022
-
- Kelliher S, Weiss L, Cullivan S, O'Rourke E, Murphy CA, Toolan S, et al. Non-severe COVID-19 is associated with endothelial damage and hypercoagulability despite pharmacological thromboprophylaxis. Journal of Thrombosis and Haemostasis 2022;[Epub ahead of print]. [DOI: 10.1111/jth.15660] - DOI - PMC - PubMed
Klok 2020a
Klok 2020b
Kyriakoulis 2022
-
- Kyriakoulis KG, Kollias A, Kyriakoulis IG, Kyprianou IA, Papachrysostomou C, Makaronis P, et al. Thromboprophylaxis in patients with COVID-19: systematic review of national and international clinical guidance reports. Current Vascular Pharmacology 2022;20(1):96-110. [PMID: ] - PubMed
Lee 2021
Lefebvre 2022
-
- Lefebvre C, Glanville J, Briscoe S, Featherstone R, Littlewood A, Marshall C, et al. Chapter 4: Searching for and selecting studies. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook.
Liberati 2009
Llitjos 2020
Lodigiani 2020
Logue 2021
Marietta 2020
Matos 2011
-
- Matos MF, Lourenço DM, Orikaza CM, Bajerl JA, Noguti MA, Morelli VM. The role of IL-6, IL-8 and MCP-1 and their promoter polymorphisms IL-6 -174GC, IL-8 -251AT and MCP-1 -2518AG in the risk of venous thromboembolism: a case-control study. Thrombosis Research 2011;128(3):216-20. [PMID: ] - PubMed
McKenzie 2021
-
- McKenzie JE, Brennan SE. Chapter 12: Synthesizing and presenting findings using other methods. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook/archive/v6.2.
Middeldorp 2020
Moores 2020
NCT04542408
-
- NCT04542408. Hamburg edoxaban for anticoagulation in COVID-19 study (HERO-19). clinicaltrials.gov/ct2/show/NCT04542408 (first received 6 September 2020).
NICE 2019
-
- National Clinical Guideline Centre. Venous thromboembolism in over 16s: reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism: NICE guideline (NG89); 2019. nice.org.uk/guidance/ng89. - PubMed
NICE 2020
-
- National Clinical Guideline Centre. Venous thromboembolic diseases: diagnosis, management and thrombophilia testing. NICE guideline (NG158); 2020. nice.org.uk/guidance/ng158.
NIH 2022
-
- Coronavirus Disease 2019 (COVID-19) Treatment Guidelines [Internet]. Bethesda (MD): National Institutes of Health (US). covid19treatmentguidelines.nih.gov/ (assessed 9 November 2022). [PMID: ] - PubMed
NIHR 2022
-
- NIHR Global Health Unit on Global Surgery, COVIDSurg Collaborative. Elective surgery system strengthening: development, measurement, and validation of the surgical preparedness index across 1632 hospitals in 119 countries. Lancet 2022;400(10363):1607-17. [DOI: 10.1016/S0140-6736(22)01846-3] - DOI - PMC - PubMed
Ortega‐Paz 2021
-
- Ortega-Paz L, Capodanno D, Montalescot G, Angiolillo DJ. Coronavirus disease 2019-associated thrombosis and coagulopathy: review of the pathophysiological characteristics and implications for antithrombotic management. Journal of the American Heart Association 2021;10(3):e019650. [PMID: ] - PMC - PubMed
Paranjpe 2020
Phelan 2020
-
- Phelan AL, Katz R, Gostin LO. The novel Coronavirus originating in Wuhan, China: challenges for global health governance. JAMA 2020;323(8):709-10. [PMID: ] - PubMed
Ramacciotti 2020
-
- Ramacciotti E, Macedo AS, Biagioni RB, Caffaro RA, Lopes RD, Guerra JC, et al. Evidence-based practical guidance for the antithrombotic management in patients with Coronavirus disease (COVID-19) in 2020. Clinical and Applied Thrombosis/Hemostasis 2020;26:1076029620936350. [DOI: 10.1177/1076029620936350] [PMID: ] - DOI - PMC - PubMed
Ramacciotti 2022
-
- Ramacciotti E, Barile Agati L, Calderaro D, Aguiar VC, Spyropoulos AC, Oliveira CC, et al. Rivaroxaban versus no anticoagulation for post-dischargethromboprophylaxis after hospitalisation for COVID-19 (MICHELLE): an open-label, multicentre, randomised, controlled trial. Lancet 2022;399(10319):50-9. [DOI: 10.1016/S0140-6736(21)02392-8] - DOI - PMC - PubMed
Reeves 2021
-
- Reeves BC, Deeks JJ, Higgins JP, Shea B, Tugwell P, Wells GA. Chapter 24: Including non-randomized studies on intervention effects. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook/archive/v6.2.
RevMan Web 2022 [Computer program]
-
- Review Manager Web (RevMan Web). Version 4.3.0. The Cochrane Collaboration, 2022. Available at revman.cochrane.org.
Righini 2006
-
- Righini M, Paris S, Le Gal G, Laroche JP, Perrier A, Bounameaux H. Clinical relevance of distal deep vein thrombosis. Review of literature data. Thrombosis and Haemostasis 2006;95(1):56-64. [PMID: ] - PubMed
Sachdeva 2014
Saposnik 2011
-
- Saposnik G, Barinagarrementeria F, Brown RD Jr, Bushnell CD, Cucchiara B, Cushman M, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011;42(4):1158-92. [PMID: ] - PubMed
Schulman 2010
-
- Schulman S, Angeras U, Bergqvist D, Eriksson B, Lassen MR, Fisher W. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in surgical patients. Journal of Thrombosis and Haemostasis 2010;8(1):202-4. [PMID: ] - PubMed
Schulman 2022
Schünemann 2021a
-
- Schünemann HJ, Higgins JP, Vist GE, Glasziou P, Akl EA, Skoetz N, et al. Chapter 14: Completing ‘Summary of findings’ tables and grading the certainty of the evidence. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook/archive/v6.2.
Schünemann 2021b
-
- Schünemann HJ, Vist GE, Higgins JP, Santesso N, Deeks JJ, Glasziou P, et al. Chapter 15: Interpreting results and drawing conclusions. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook/archive/v6.2.
Shah 2021
-
- Shah W, Hillman T, Playford ED, Hishmeh L. Managing the long term effects of covid-19: summary of NICE, SIGN, and RCGP rapid guideline. BMJ (Clinical research ed.) 2021;372:n136. [PMID: ] - PubMed
Sobreira 2020
Spyropoulos 2011
-
- Spyropoulos AC, Anderson FA Jr, FitzGerald G, Decousus H, Pini M, Chong BH, et al. Predictive and associative models to identify hospitalized medical patients at risk for VTE. Chest 2011;140(3):706-14. [PMID: ] - PubMed
Spyropoulos 2018
Spyropoulos 2020
-
- Spyropoulos AC, Levy JH, Ageno W, Connors JM, Hunt BJ, Iba T, et al. Scientific and Standardization Committee communication: clinical guidance on the diagnosis, prevention, and treatment of venous thromboembolism in hospitalized patients with COVID-19. Journal of Thrombosis and Haemostasis 2020;18(8):1859-65. [PMID: ] - PMC - PubMed
Spyropoulos 2022
-
- Spyropoulos AC, Connors JM, Douketis JD, Goldin M, Hunt BJ, Kotila TR, et al. Good practice statements for antithrombotic therapy in the management of COVID-19: guidance from the SSC of the ISTH. Journal of Thrombosis and Haemostasis 2022;20(10):2226-36. [DOI: 10.1111/jth.15809] - DOI - PMC - PubMed
Stein 1991
-
- Stein PD, Saltzman HA, Weg JG. Clinical characteristics of patients with acute pulmonary embolism. American Journal of Cardiology 1991;68(17):1723-4. [PMID: ] - PubMed
Sterne 2017
-
- Sterne JA, Egger M, Moher D, Boutron I, editor(s). Chapter 10: Addressing reporting biases. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.2.0 (updated June 2017). Cochrane, 2017. Available from training.cochrane.org/handbook/archive/v5.2.
Tang 2020
Tomidokoro 2021
Townsend 2021
Tsaplin 2021
Tunjungputri 2022
-
- Tunjungputri RN, Tetrasiwi EN, Mulansari NA, Harimurti K, Nelwan EJ. Parenteral and oral anticoagulant treatment for hospitalized and post-discharge COVID-19 patients: a systematic review and meta-analysis. Acta Medica Indonesiana 2022;54(2):190-209. [PMID: ] - PubMed
Valla 2002
-
- Valla DC, Condat B, Lebrec D. Spectrum of portal vein thrombosis in the west. Journal of Gastroenterology and Hepatology 2002;17(Suppl 3):S224-7. [PMID: ] - PubMed
Varga 2020
Verso 2003
-
- Verso M, Agnelli G. Venous thromboembolism associated with long-term use of central venous catheters in cancer patients. Journal of Clinical Oncology 2003;21(19):3665-75. [PMID: ] - PubMed
Wan 2014
Ware 1992
-
- Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Medical Care 1992;30(6):473-83. [PMID: ] - PubMed
Weitz 2017
WHO 2020
-
- World Health Organization. Protocol: real-time RT-PCR assays for the detection of SARS-CoV-2. who.int/docs/default-source/coronaviruse/real-time-rt-pcr-assays-for-the... (accessed 4 August 2021).
References to other published versions of this review
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous