

Improvement in OCD symptoms associated with serotoninergic psychedelics: a retrospective online survey
- PMID: 37591906
- PMCID: PMC10435518
- DOI: 10.1038/s41598-023-39812-0
Improvement in OCD symptoms associated with serotoninergic psychedelics: a retrospective online survey
Abstract
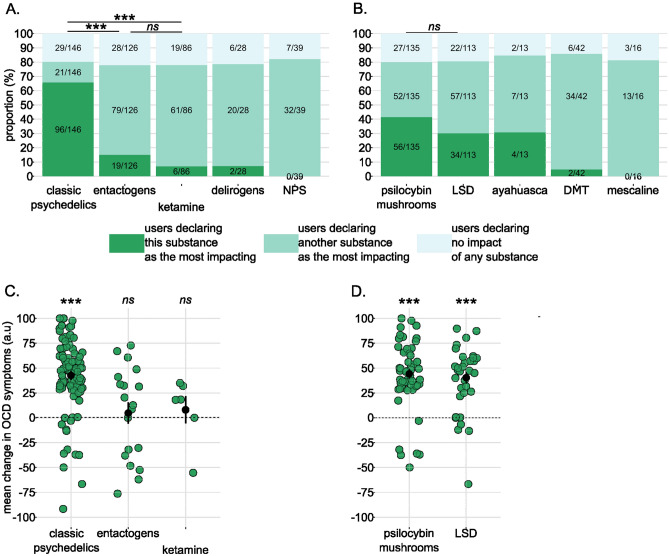
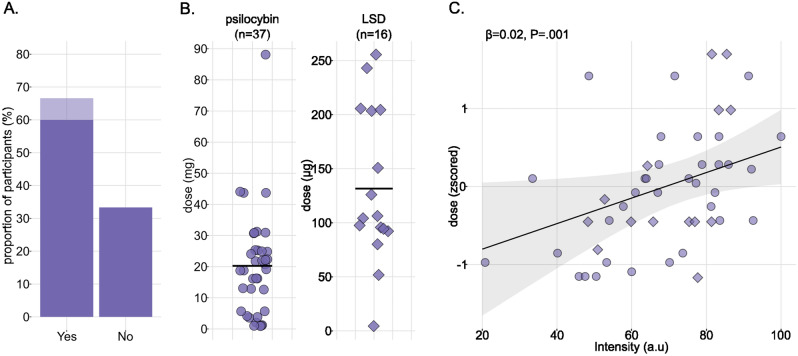
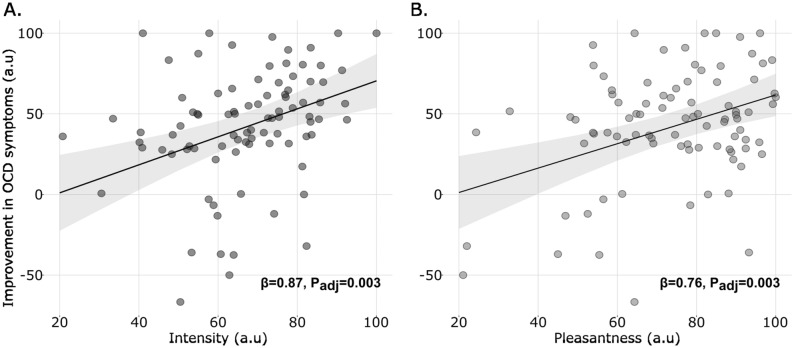
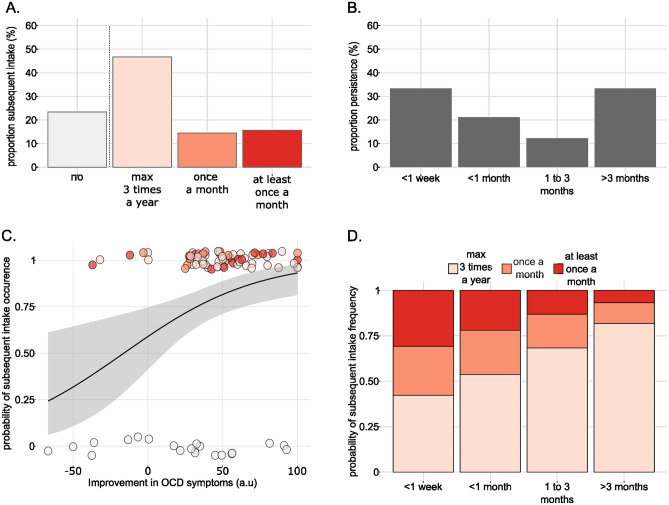
A renewed interest in the use of psychedelics for treating obsessive compulsive disorder (OCD) has emerged in the last 20 years. But pre-clinical and clinical evidence remain scarce, and little is known about the factor determining the magnitude and persistence of the therapeutic effect. We therefore designed a retrospective online survey to explore, in the general population using psychoactive drugs, their impact on OCD symptoms. We also assessed the attitude of the participants towards the substance in term of frequency of intakes. In a sample of 174 participants, classic psychedelics were reported as the only substances effective at reducing OCD symptoms. In classic psychedelics users, symptoms reduction was associated with the intensity of acute effects, itself correlated to the dose. Reports on the persistence of the therapeutic effect varied from weeks to months, but we could not find any predicting factor. Finally, the occurrence and frequency of subsequent intakes, which seemed to be limited in our sample, were predicted by the magnitude and persistence of the therapeutic effect, respectively. Our observations support the hypothesis of classic psychedelics efficacy in reducing OCD symptoms but a careful evaluation of the persistence of this effect is still needed.
© 2023. Springer Nature Limited.
Conflict of interest statement
AB, CP, AO, CD, EB, JFADS, KN, PS and MM declared no competing interests. MJ is a co-founding member of Eleusis (Psychedelic Society of French-speaking Switzerland) and SSMP (Swiss Society for Psychedelic Medicine) and board member of the Swiss Institute for Noetic Science (ISSNOE). VV and BW are president and member of the administration committee of the French psychedelic society, respectively (unpaid positions). LM is part of the Psychedelic medicine section of the AFPBN (French association for biological medicine and neuropsychopharmacology).
Figures

References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed., text rev.). (2022) doi:10.1176/appi.books.9780890425787.
-
- Abramowitz JS, Taylor S, McKay D. Obsessive-compulsive disorder. Lancet. 2009;374:491–499. - PubMed
-
- Hirschtritt ME, Bloch MH, Mathews CA. Obsessive-compulsive disorder: Advances in diagnosis and treatment. JAMA. 2017;317:1358–1367. - PubMed
-
- Visser-Vandewalle V, et al. Deep brain stimulation for obsessive–compulsive disorder: a crisis of access. Nat. Med. 2022;28:1529–1532. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
