

Baseline innate and T cell populations are correlates of protection against symptomatic influenza virus infection independent of serology
- PMID: 37592015
- PMCID: PMC10566627
- DOI: 10.1038/s41590-023-01590-2
Baseline innate and T cell populations are correlates of protection against symptomatic influenza virus infection independent of serology
Abstract
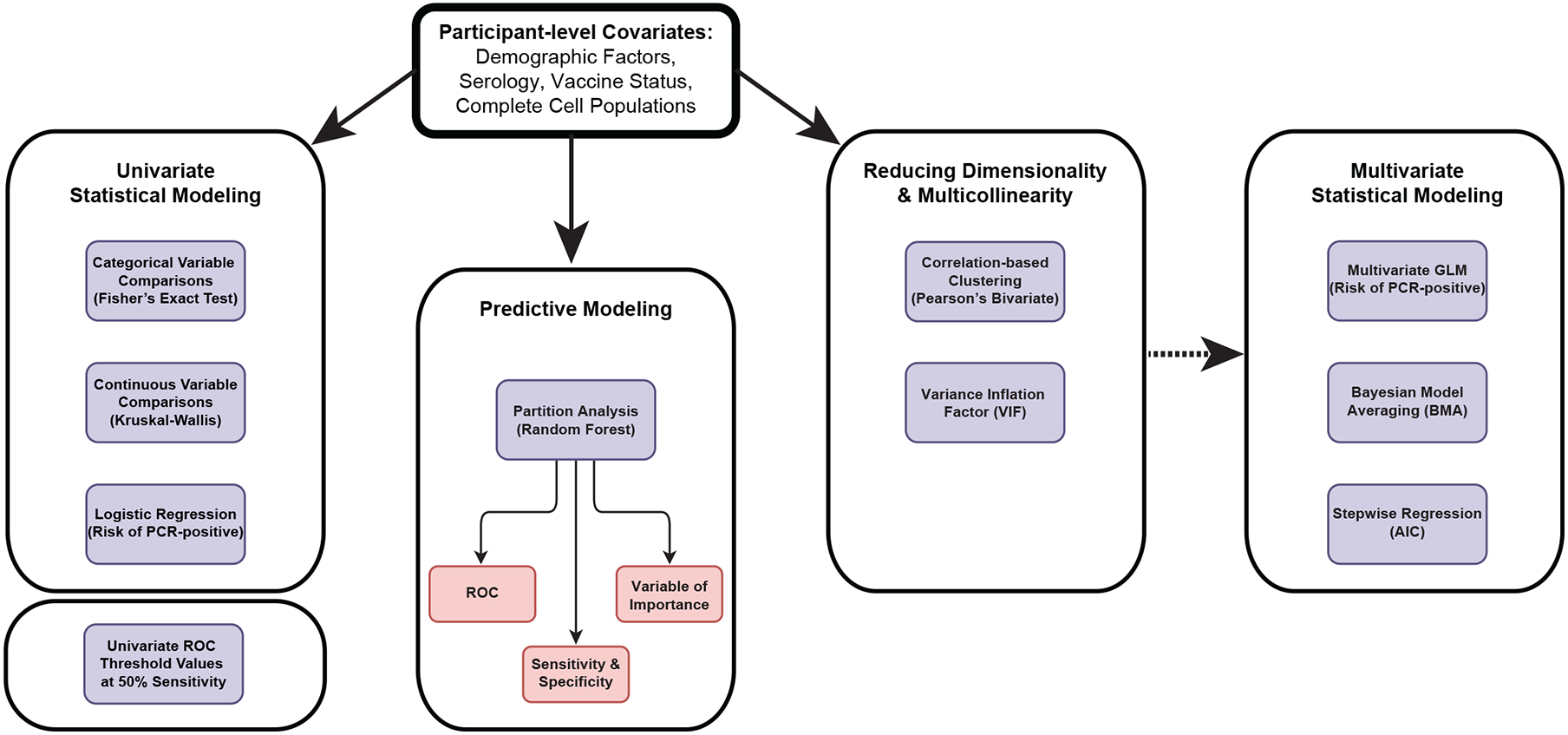
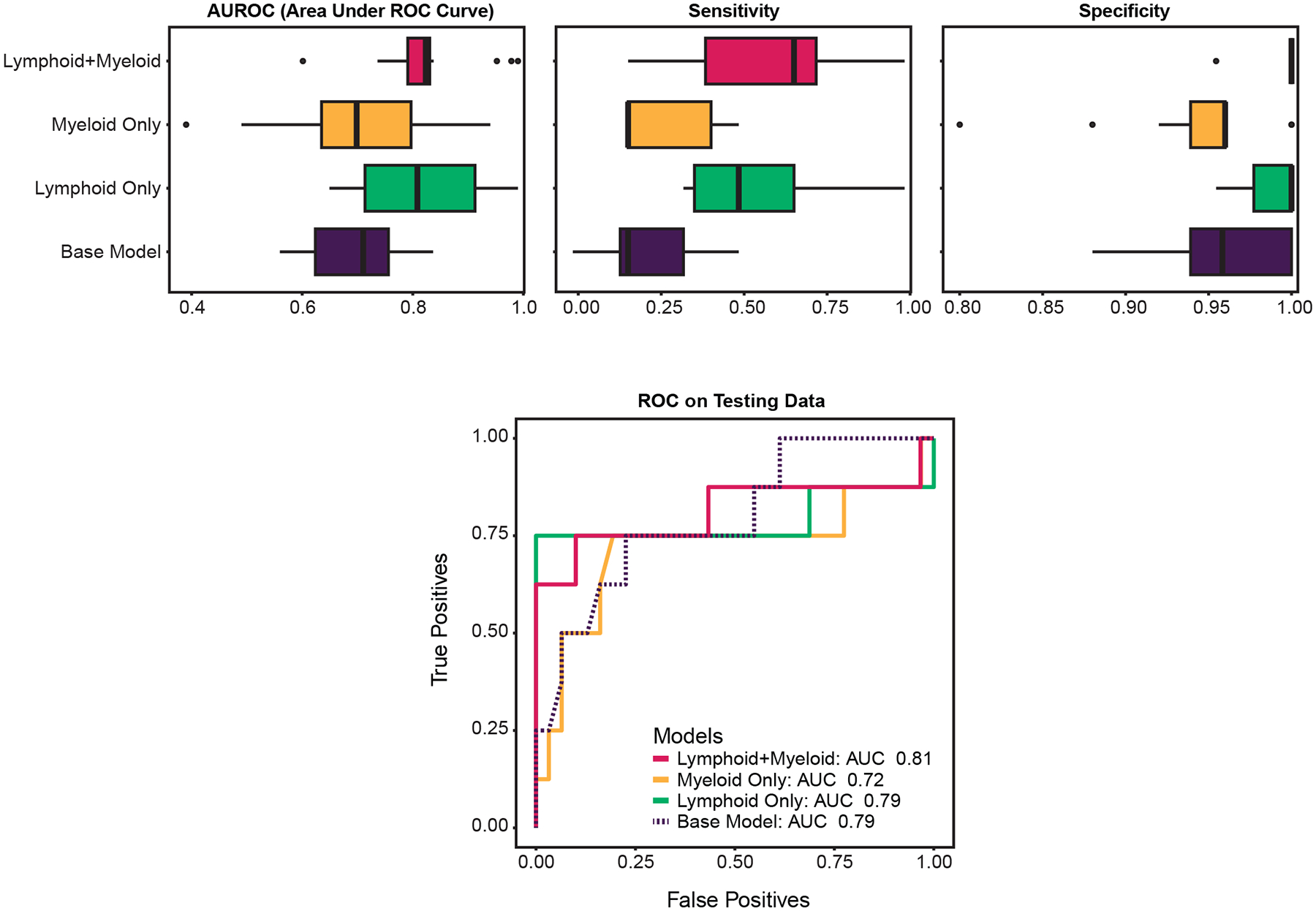
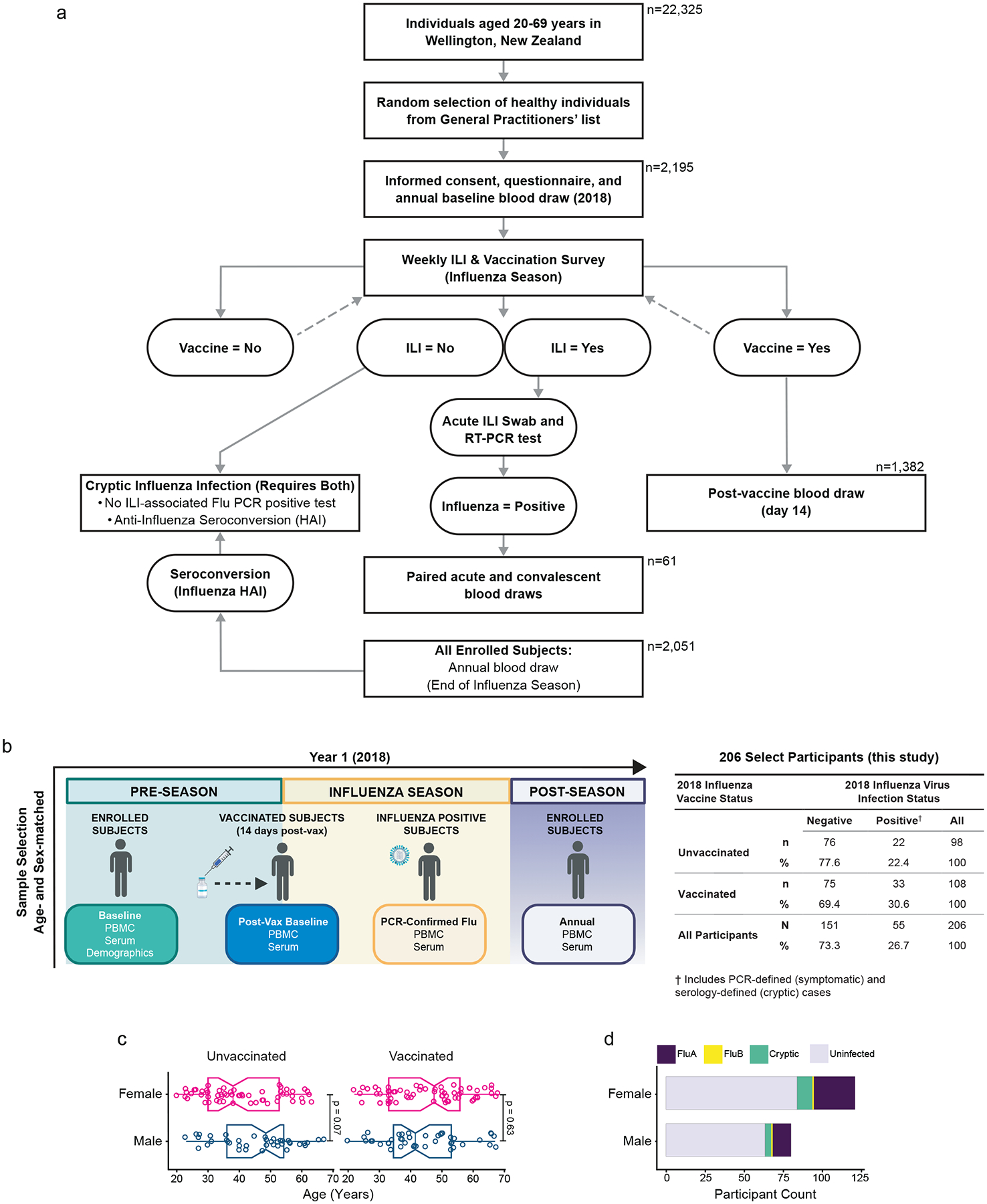
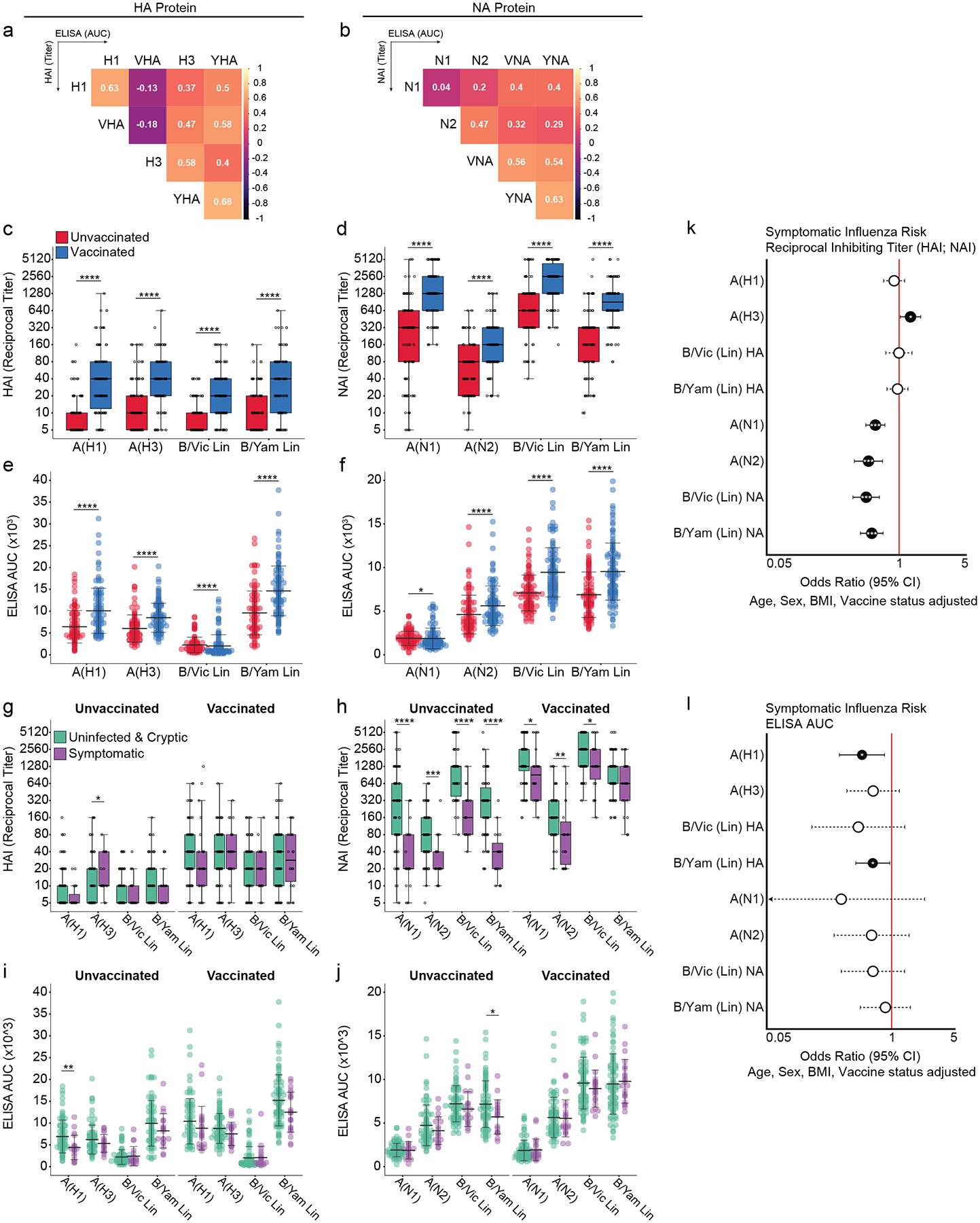
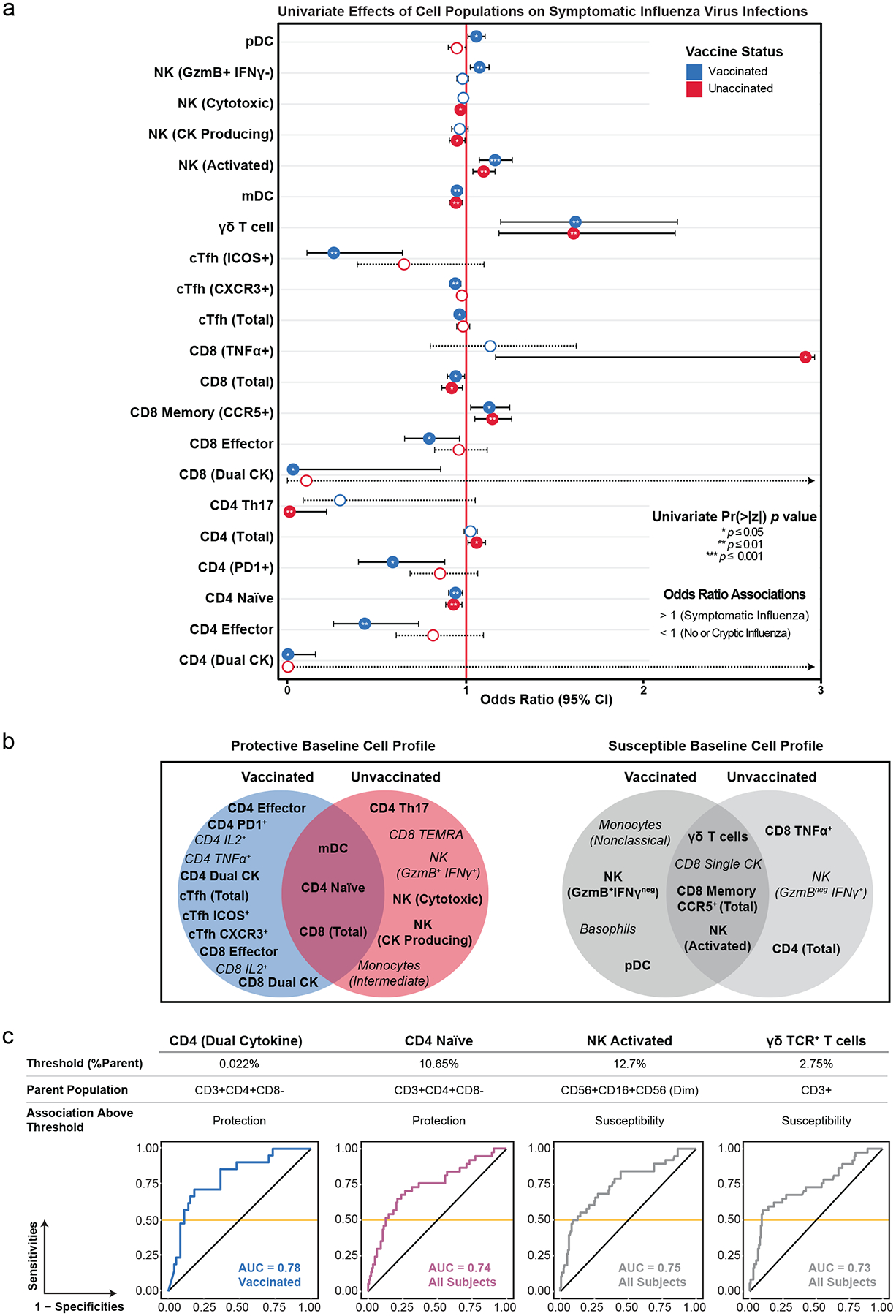
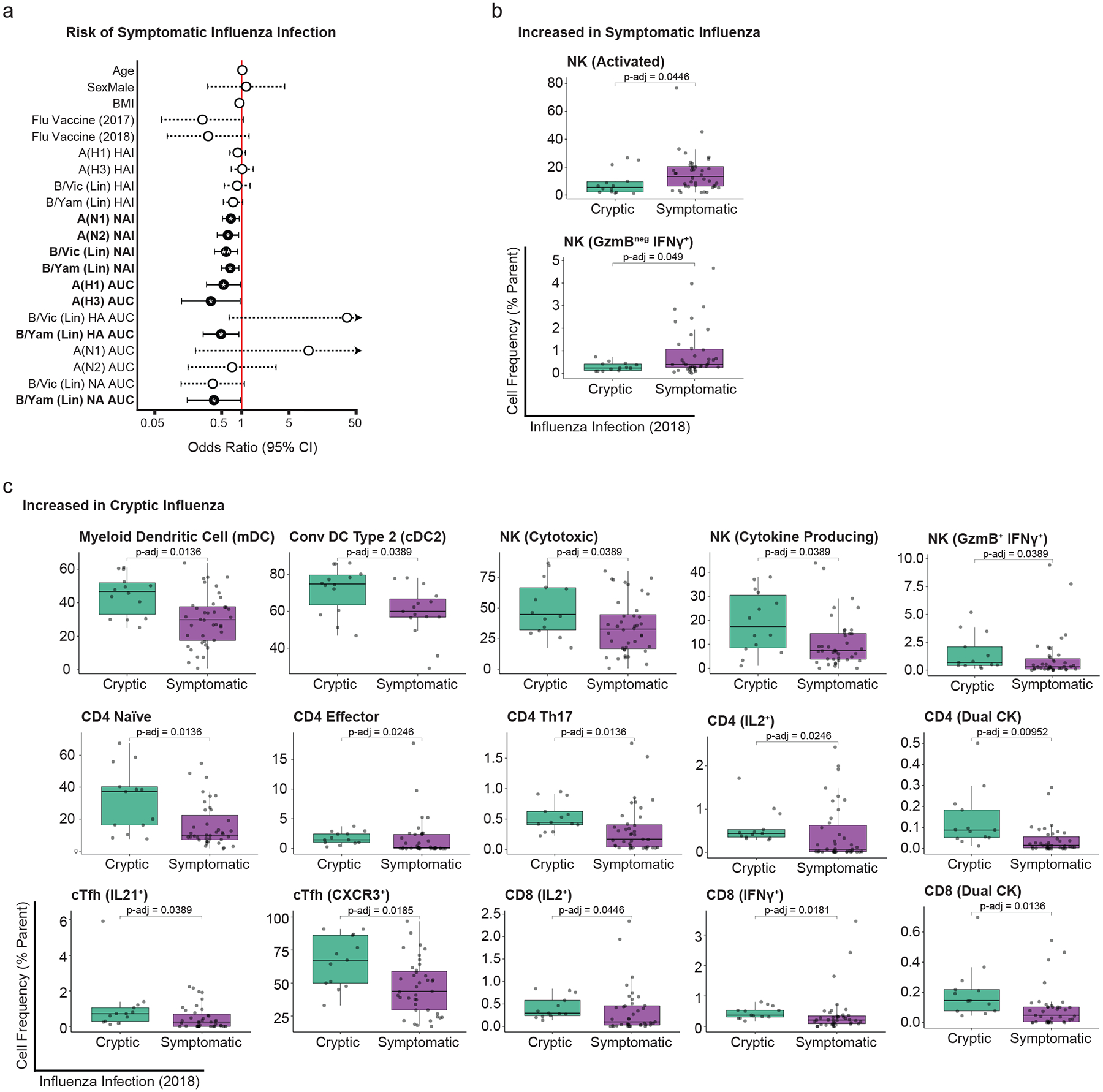
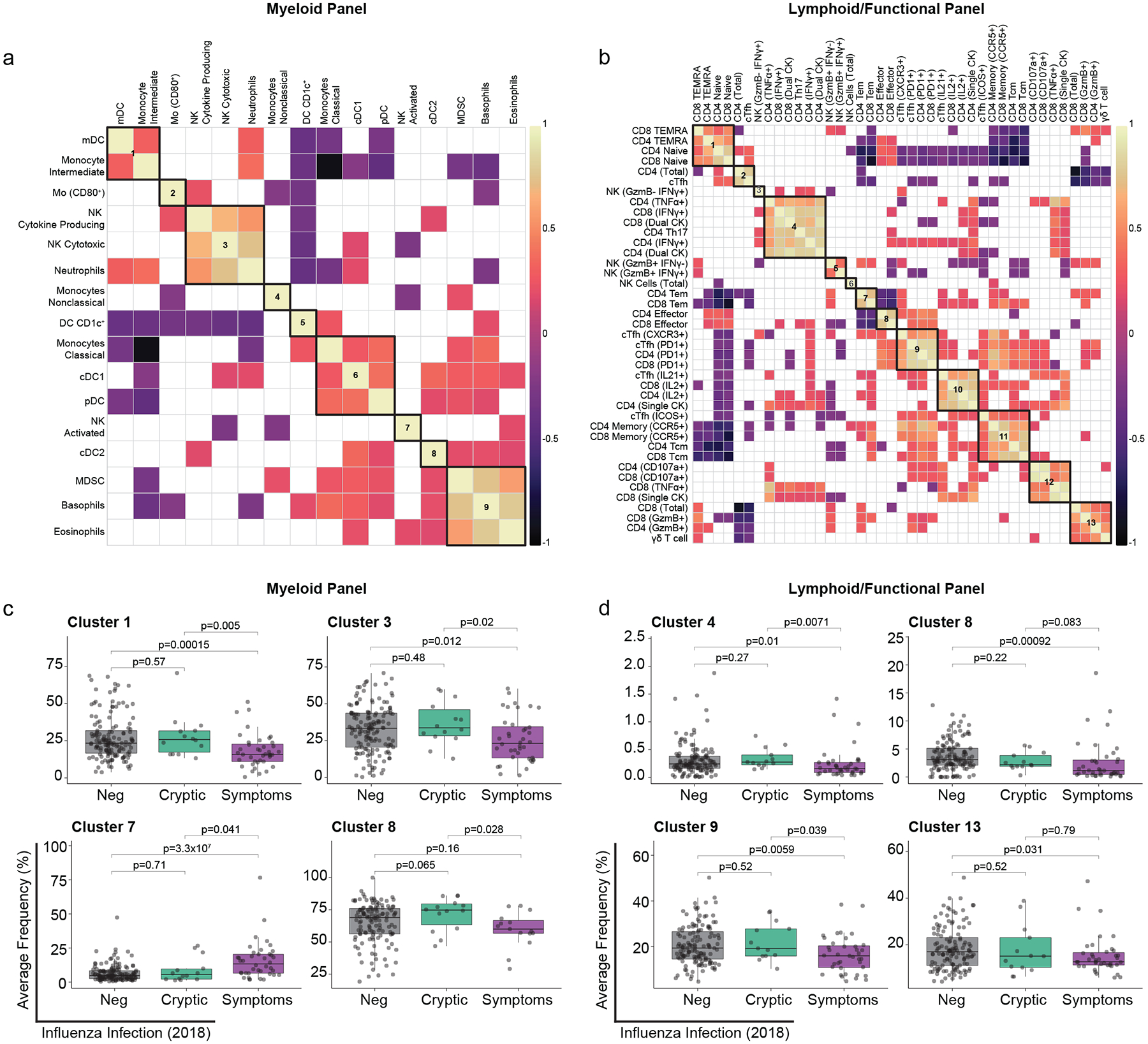
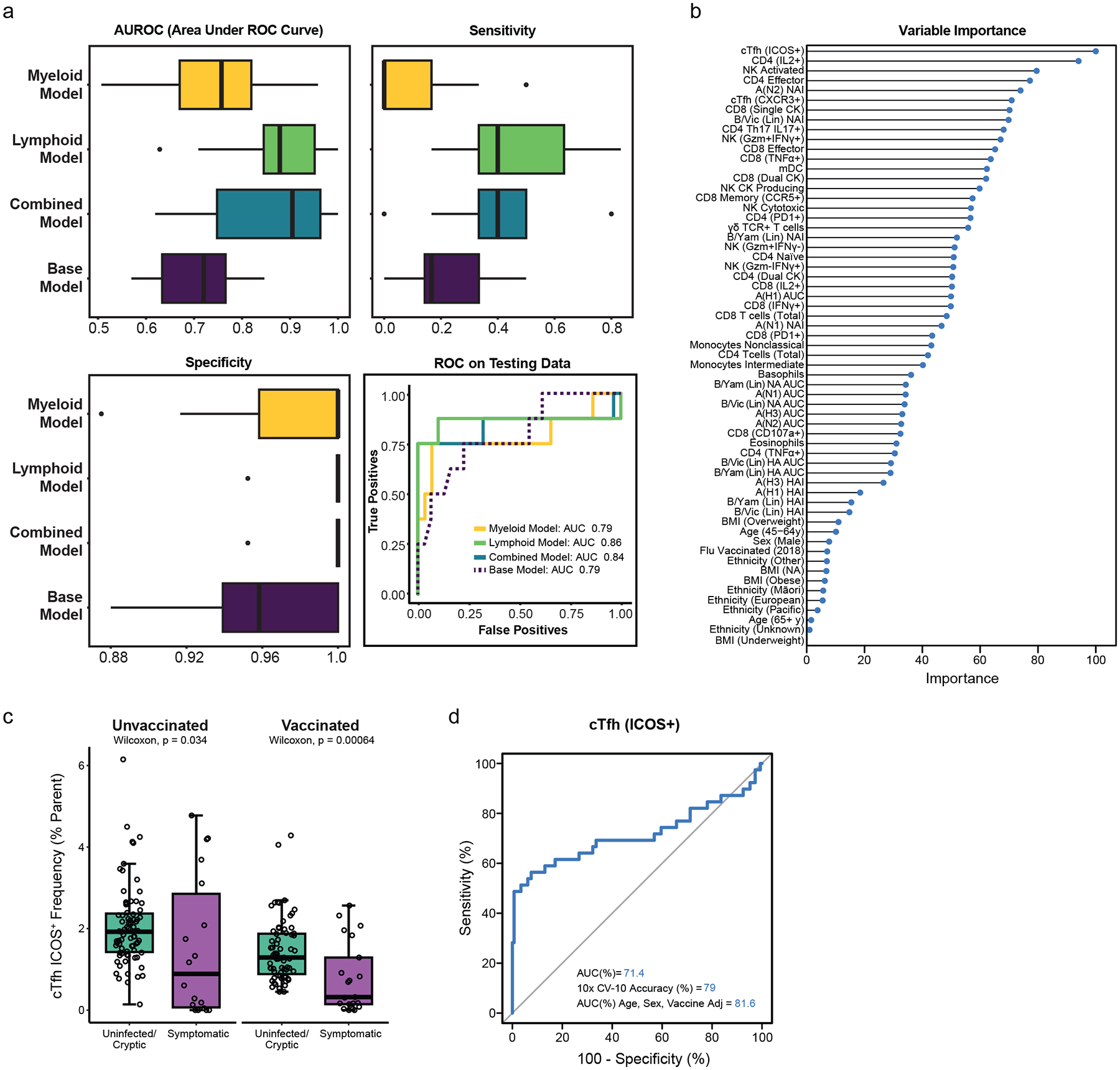
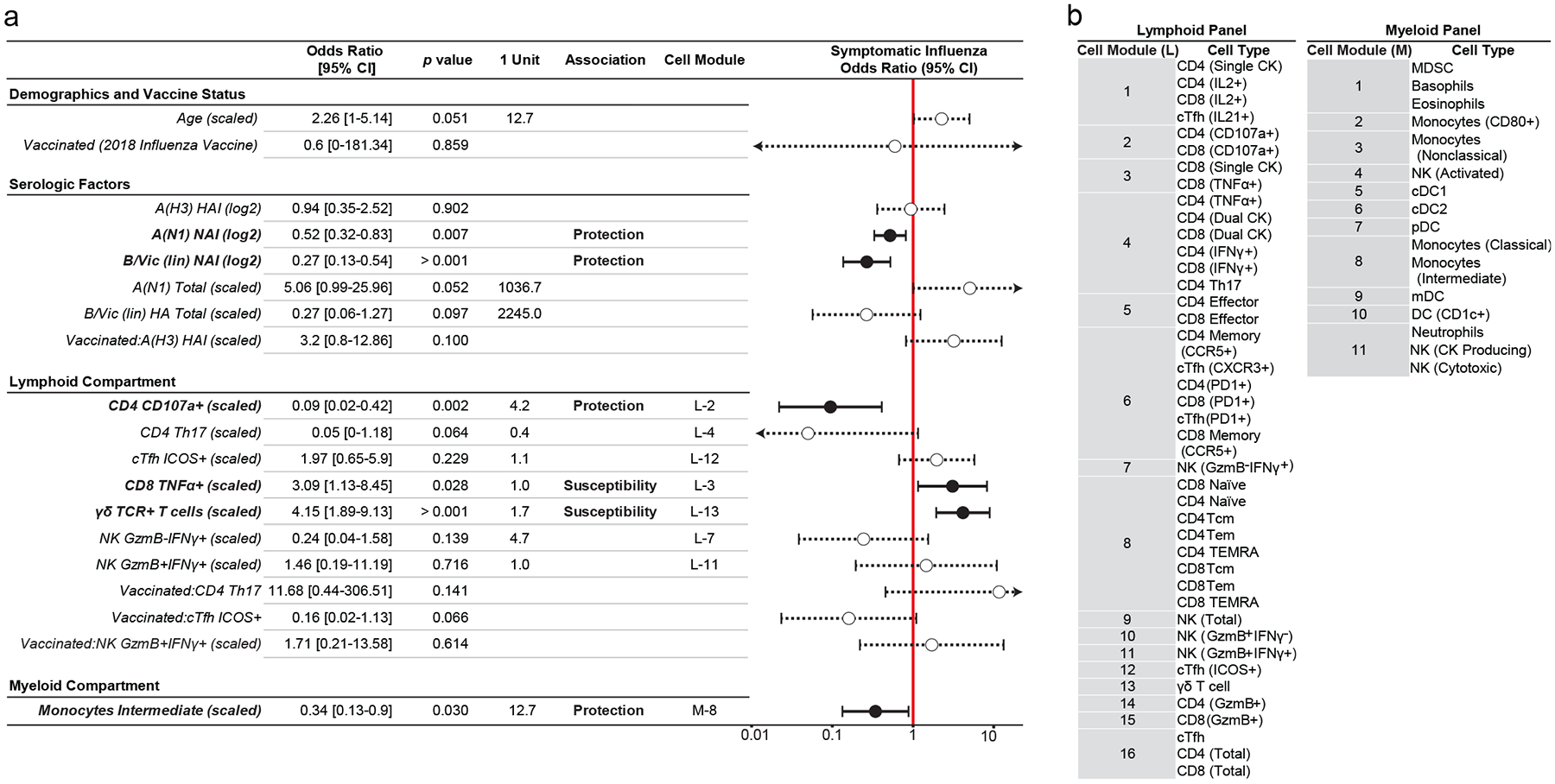
Evidence suggests that innate and adaptive cellular responses mediate resistance to the influenza virus and confer protection after vaccination. However, few studies have resolved the contribution of cellular responses within the context of preexisting antibody titers. Here, we measured the peripheral immune profiles of 206 vaccinated or unvaccinated adults to determine how baseline variations in the cellular and humoral immune compartments contribute independently or synergistically to the risk of developing symptomatic influenza. Protection correlated with diverse and polyfunctional CD4+ and CD8+ T, circulating T follicular helper, T helper type 17, myeloid dendritic and CD16+ natural killer (NK) cell subsets. Conversely, increased susceptibility was predominantly attributed to nonspecific inflammatory populations, including γδ T cells and activated CD16- NK cells, as well as TNFα+ single-cytokine-producing CD8+ T cells. Multivariate and predictive modeling indicated that cellular subsets (1) work synergistically with humoral immunity to confer protection, (2) improve model performance over demographic and serologic factors alone and (3) comprise the most important predictive covariates. Together, these results demonstrate that preinfection peripheral cell composition improves the prediction of symptomatic influenza susceptibility over vaccination, demographics or serology alone.
© 2023. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
P.G.T. has consulted or received honorarium and/or travel support from Illumina, JNJ, Pfizer, and 10X. P.G.T. serves on the Scientific Advisory Board of ImmunoScape and CytoAgents. The remaining authors declare no competing interests.
Figures



References
-
- CDC. Estimated Influenza Illnesses, Medical visits, Hospitalizations, and Deaths in the United States — 2017–2018 influenza season. Influenza (Flu) https://www.cdc.gov/flu/about/burden/2017–2018.htm#Table1 (2018).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
