

Ipilimumab with or without nivolumab in PD-1 or PD-L1 blockade refractory metastatic melanoma: a randomized phase 2 trial
- PMID: 37592104
- PMCID: PMC10708907
- DOI: 10.1038/s41591-023-02498-y
Ipilimumab with or without nivolumab in PD-1 or PD-L1 blockade refractory metastatic melanoma: a randomized phase 2 trial
Abstract
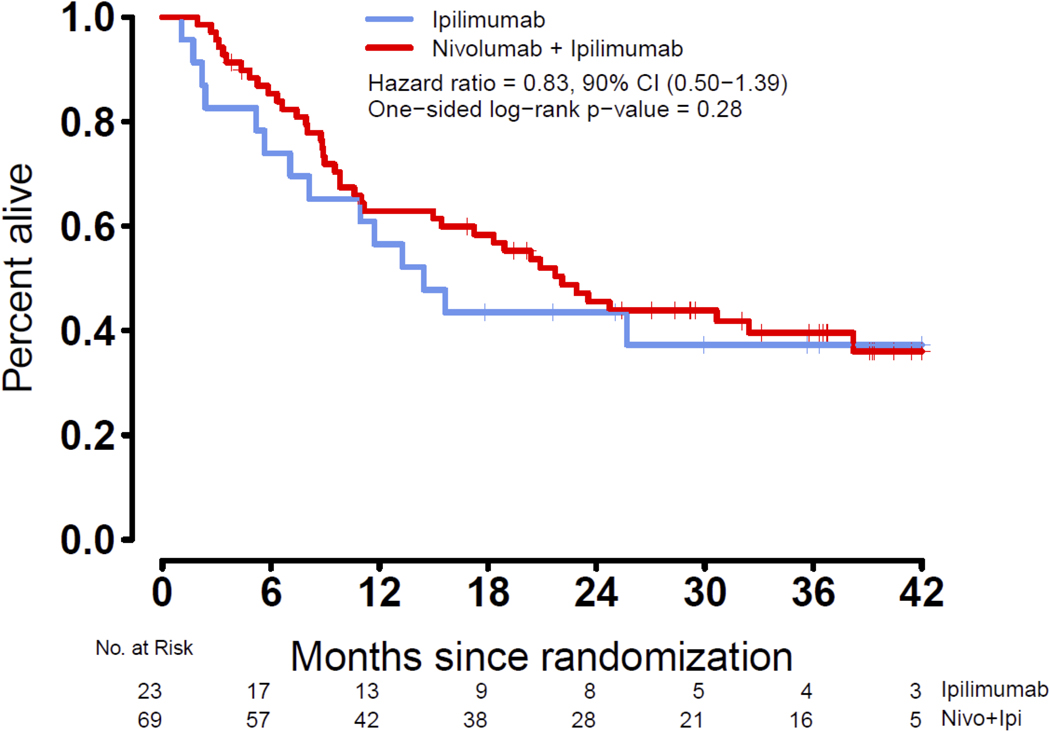
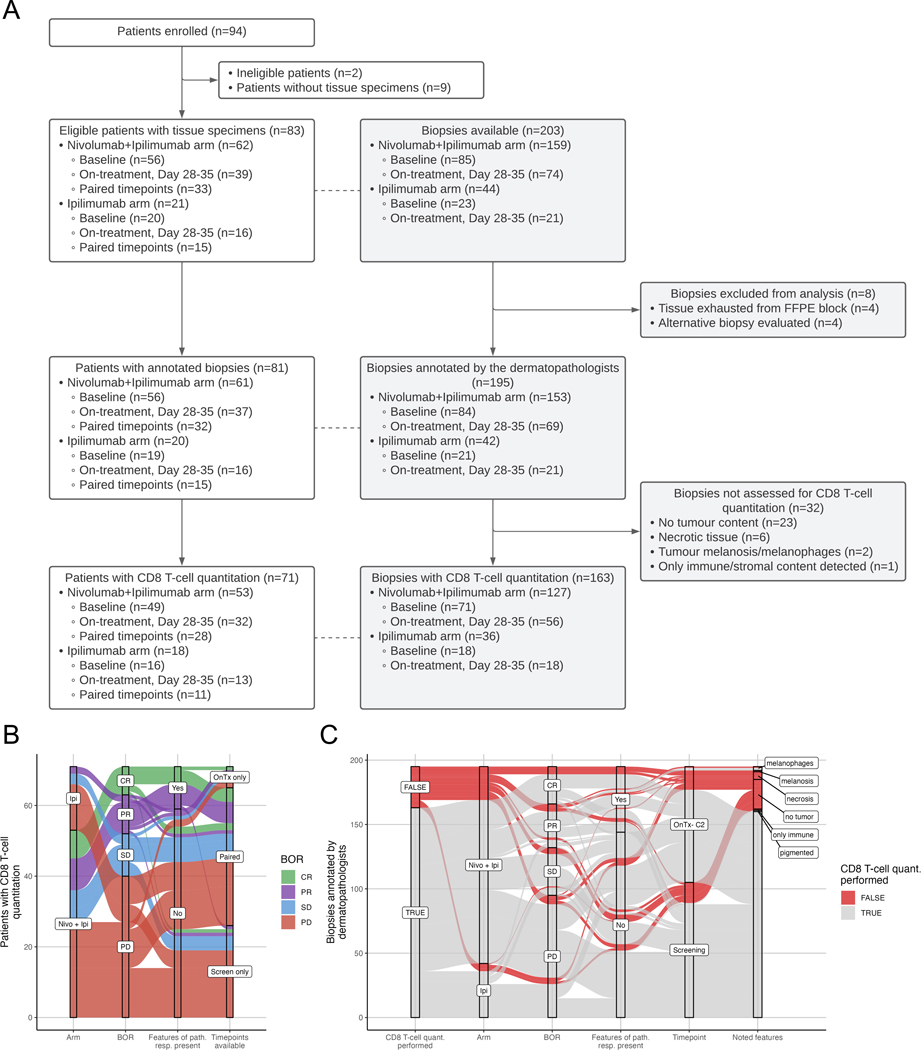
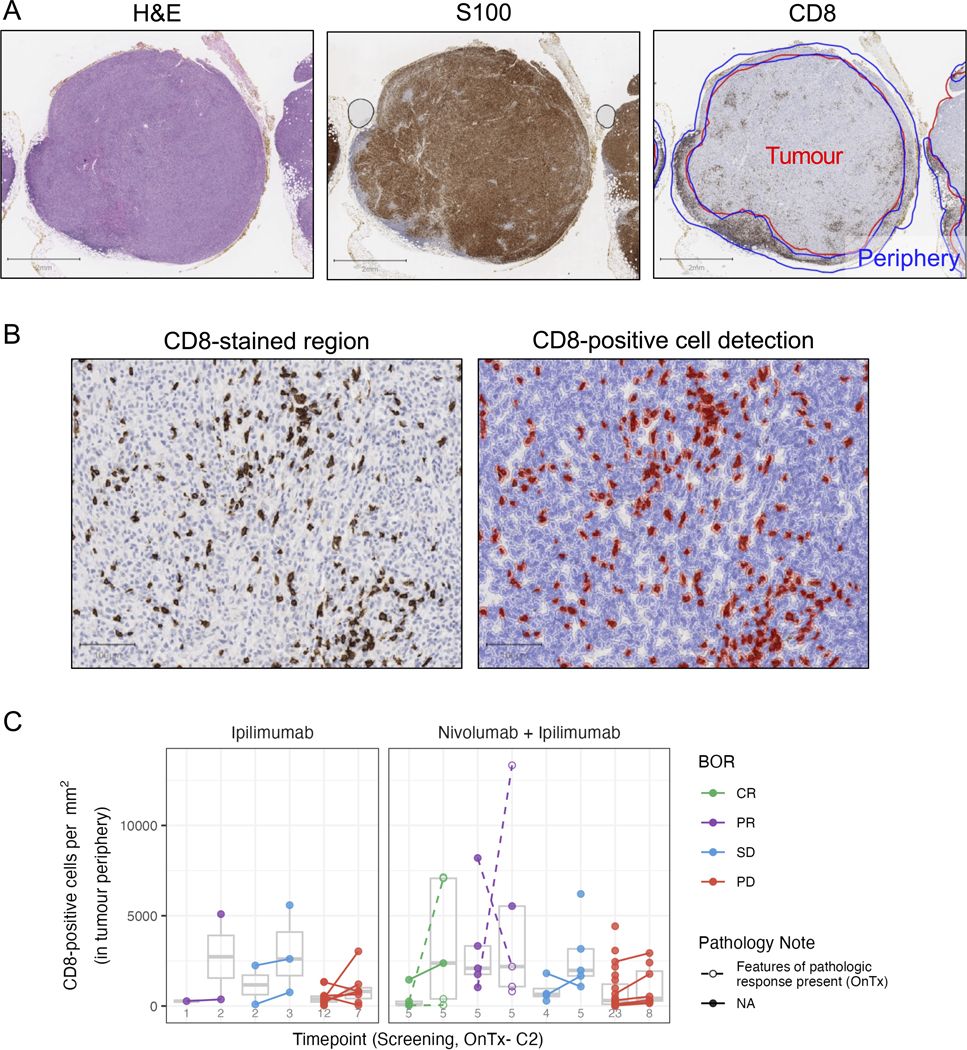
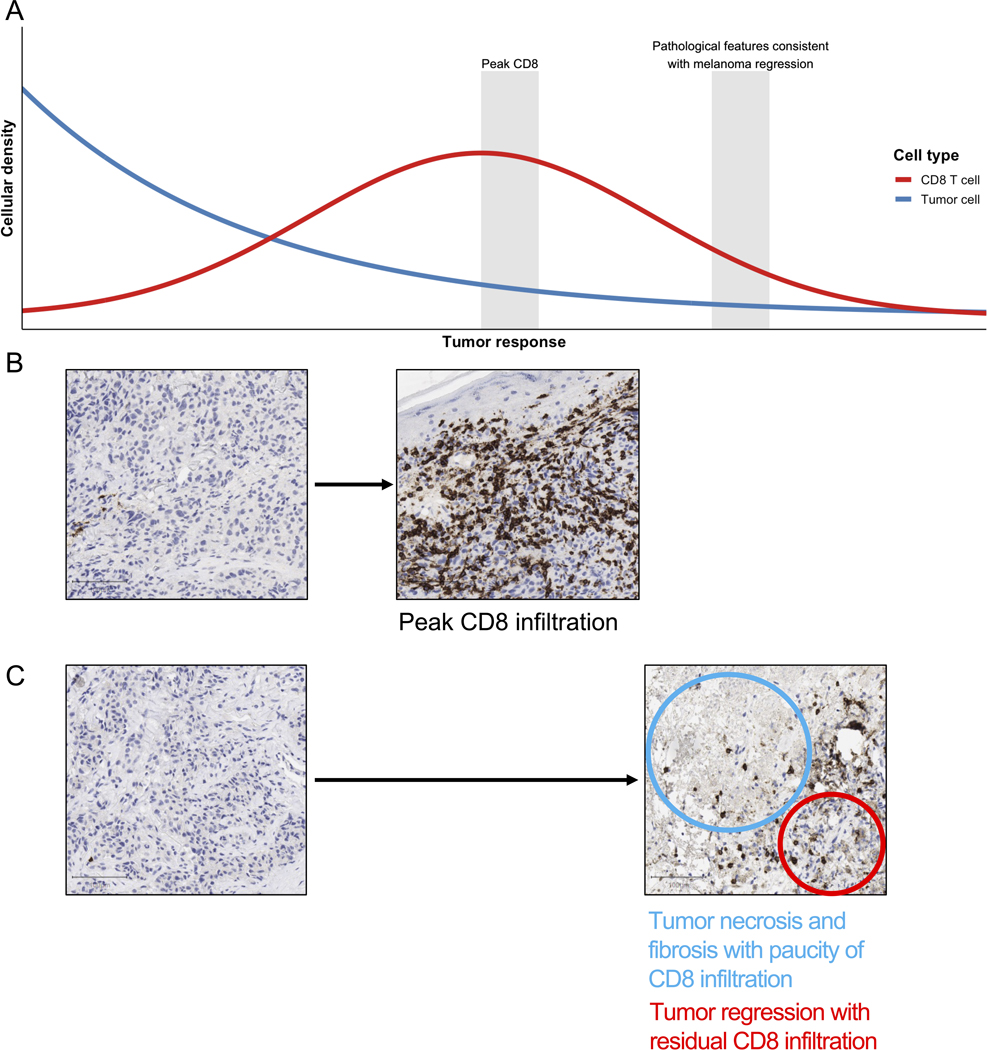
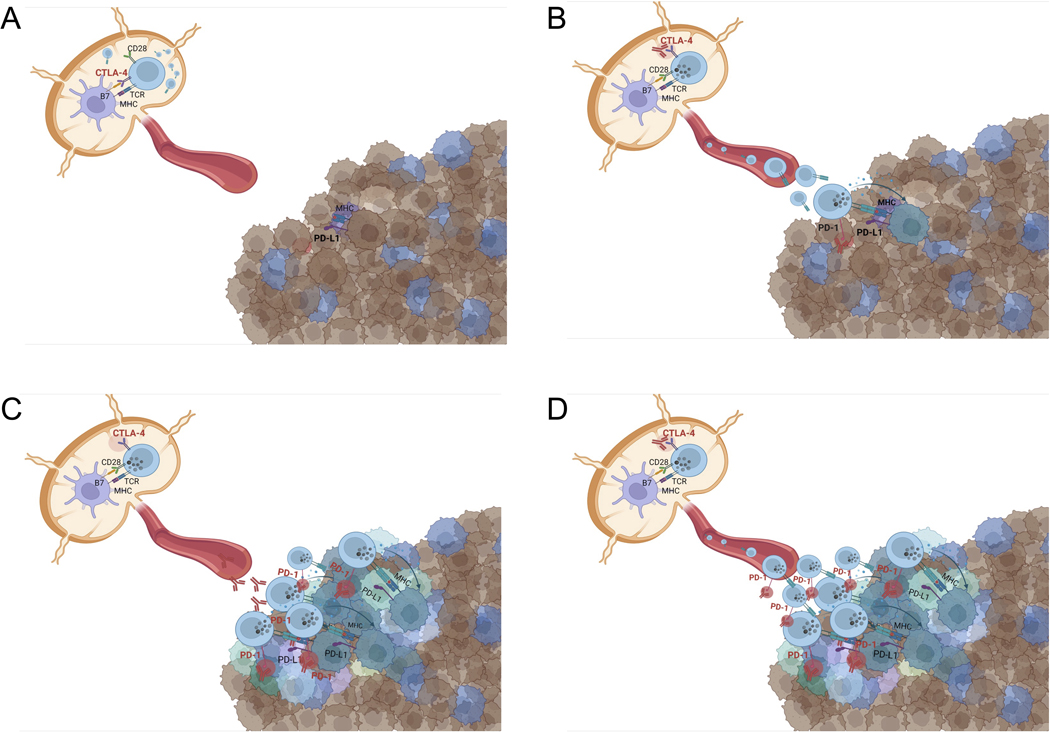
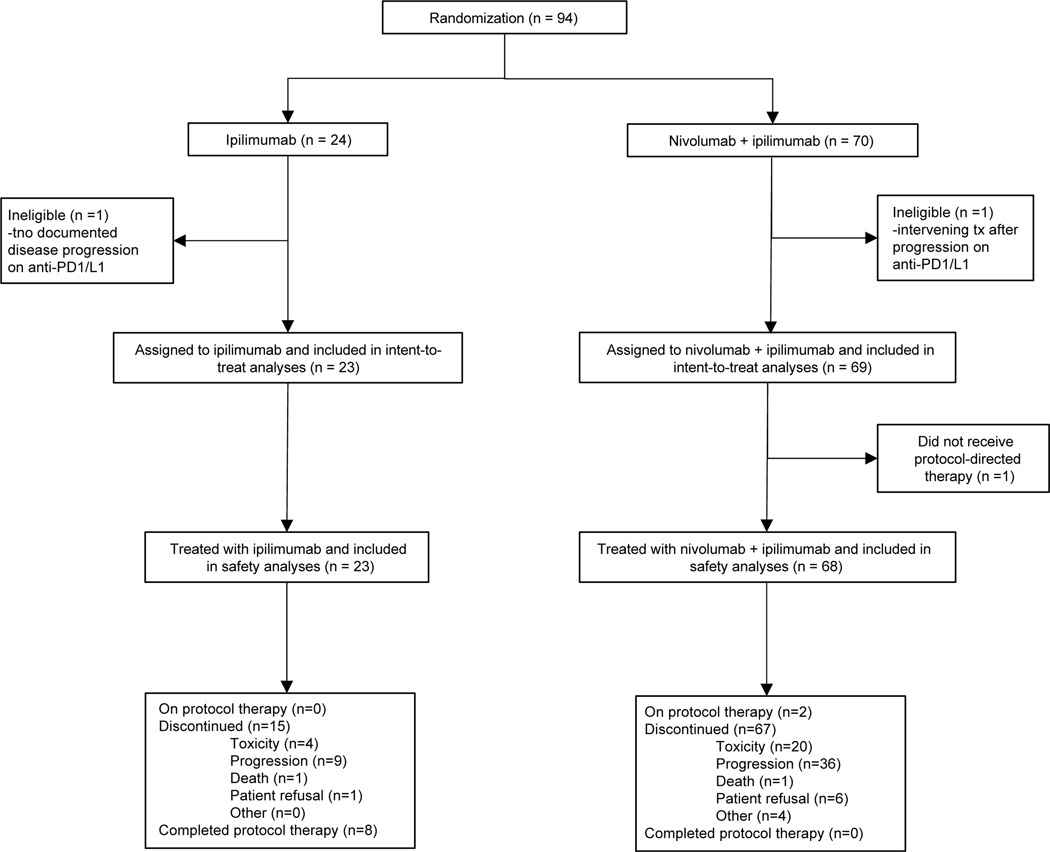
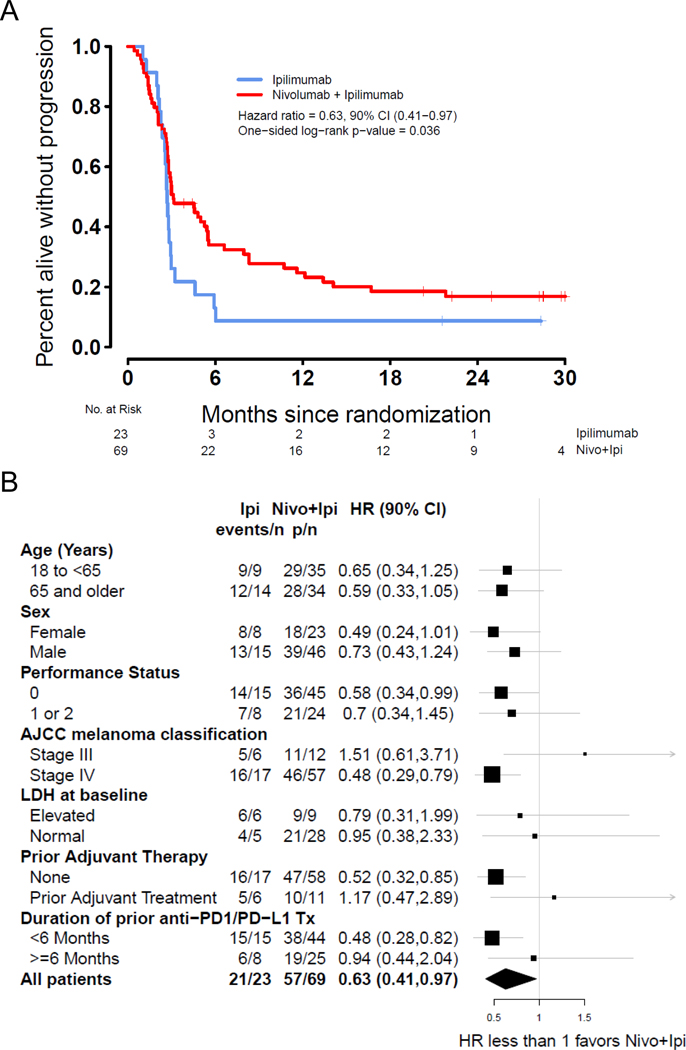
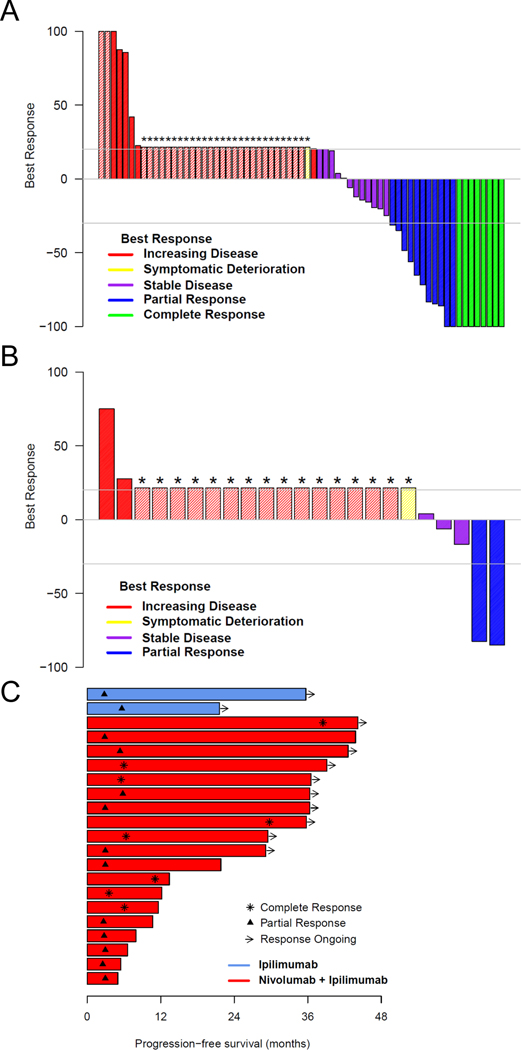
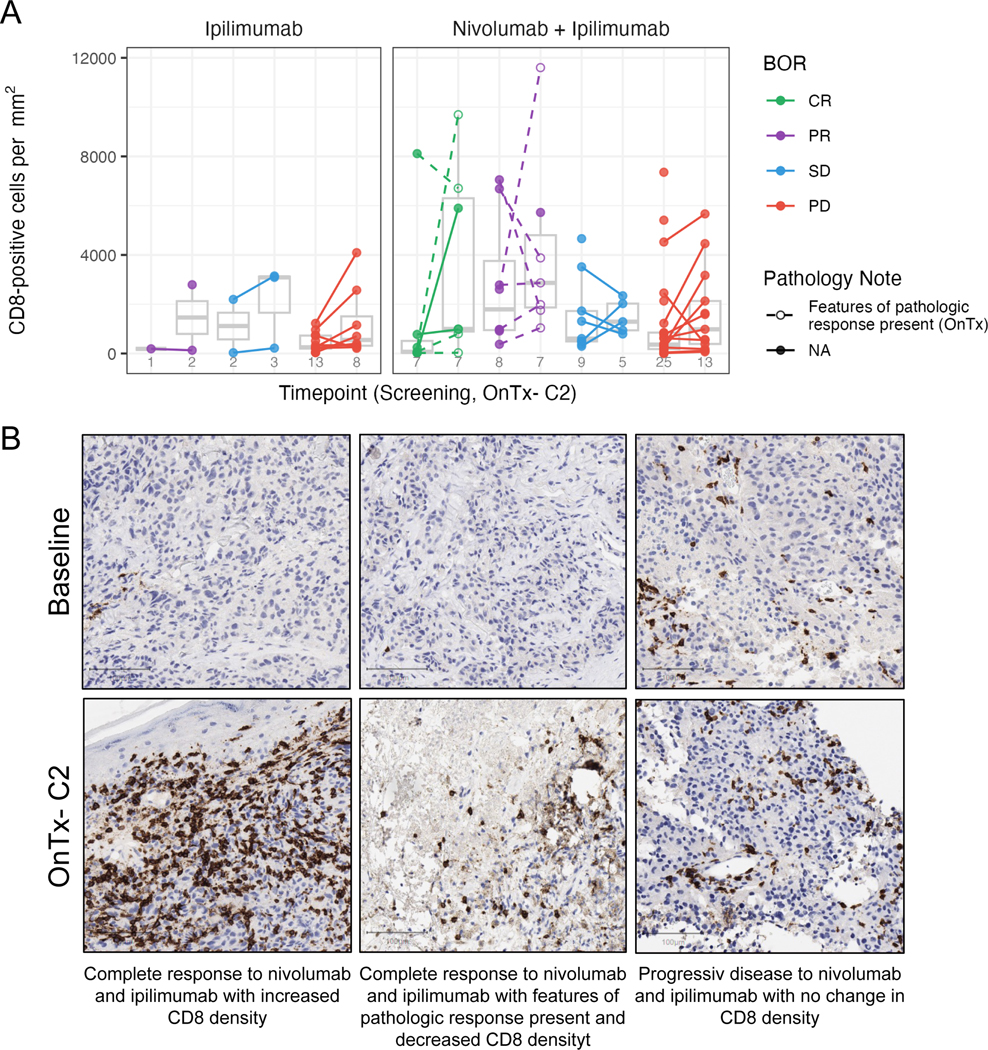
In this randomized phase 2 trial, blockade of cytotoxic T-lymphocyte protein 4 (CTLA-4) with continuation of programmed death protein 1 (PD-1) blockade in patients with metastatic melanoma who had received front-line anti-PD-1 or therapy against programmed cell death 1 ligand 1 and whose tumors progressed was tested in comparison with CTLA-4 blockade alone. Ninety-two eligible patients were randomly assigned in a 3:1 ratio to receive the combination of ipilimumab and nivolumab, or ipilimumab alone. The primary endpoint was progression-free survival. Secondary endpoints included the difference in CD8 T cell infiltrate among responding and nonresponding tumors, objective response rate, overall survival and toxicity. The combination of nivolumab and ipilimumab resulted in a statistically significant improvement in progression-free survival over ipilimumab (hazard ratio = 0.63, 90% confidence interval (CI) = 0.41-0.97, one-sided P = 0.04). Objective response rates were 28% (90% CI = 19-38%) and 9% (90% CI = 2-25%), respectively (one-sided P = 0.05). Grade 3 or higher treatment-related adverse events occurred in 57% and 35% of patients, respectively, which is consistent with the known toxicity profile of these regimens. The change in intratumoral CD8 T cell density observed in the present analysis did not reach statistical significance to support the formal hypothesis tested as a secondary endpoint. In conclusion, primary resistance to PD-1 blockade therapy can be reversed in some patients with the combination of CTLA-4 and PD-1 blockade. Clinicaltrials.gov identifier: NCT03033576 .
© 2023. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
A.V. declares that he has employment by Caris Life Sciences, and consults with George Clinical, West Clinic; Advisory Boards and Steering Committees: Bristol Myers Squibb, Genentech, Mirati Therapeutics; Research Funding: SWOG, Stand Up 2 Cancer, Bristol Myers Squibb, AACR.
J.M. reports none.
K.K. reports clinical trial funding through the institution from Merck.
N.I.K. reports the following: Advisory Board: Bristol Myers-Squibb, Regeneron, Merck, Iovance Biotherapeutics, Genzyme, Novartis, Nektar, Castle Biosciences, Instil Bio, NCCN (via Pfizer); Study Steering Committee: Bristol Myers-Squibb, Nektar, Regeneron, Replimmune; Data Safety Monitoring Board: Astra-Zeneca, Incyte; Common Stock: Bellicum, Asensus Surgical, Amarin Corp.; Research Funding (to Institute): Bristol Myers-Squibb, Merck, Novartis, GlaxoSmithKline, HUYA Bioscience, Amgen, Regeneron, Celgene, Replimmune, Modulation Therapeutics.
K.M.C. reports being a shareholder in Geneoscopy LLC, and has received consulting fees from Geneoscopy LLC, PACT Pharma, Tango Therapeutics, Flagship Labs 81 LLC, and the Rare Cancer Research Foundation.
P.S. received research funding, consulted for, and served on advisory board for Castle Biosciences, Inc.
L.F.K. reports none.
F.C. reports that his institution receives research funding for clinical trials. A portion of that funding comes from trials sponsored by Amgen and Replimune and helps cover her salary.
J.A.S. reports the following: Apixagen Consultation; Iovance: Consultation; Necktor: Consultation. Up-to Date: Royalties
A.I. discloses research funding to institution: Checkmate Pharmaceuticals, Dynavax, GSK/Sarah Cannon, Immunocore, Merck, Neon Therapeutics/Sarah Cannon.
A.I.V. reports that she did have an investigator-initiated study supported by Bristol Myers Squibb, but that it closed 2 years ago and understands that it does not qualify as a conflict of interest.
T-G.T. reports institutional funding from BMS, Merck, Roche, Pfizer, Novartis, Regeneron, Astra-Zeneca TGT.
B.C. reported clinical trial support paid to Institution: SWOG, BMS, Macrogenics, Merck, Karyopharm, Infinity, Advenchen, Idera, Xencor, Compugen, Iovance, PACT Pharma, RAPT, Immunocore, IDEAYA, Ascentage, Novartis, Atreca, Replimmune, Instil Bio, Adagene, TriSalus, Xilio; Payment for lecture: Sanofi Genzyme; Advisory Board: Instil Bio, Nektar, Delcath, Novartis, Genentech, IDEAYA, OncoSec, Iovance, Deciphera
D.C.P. reports none.
Y.C. reports BMS RELATIVITY-098 research funding to his institution; Personal financial interest: -BMS melanoma speaker and advisory board; -Pfizer melanoma speaker.
K.M. reports no relevant competing interests.
C.L.B. reports none.
C.A.D. reports no conflicts of interest or any relationships to declare.
D.B.J. has served on advisory boards or as a consultant for BMS, Catalyst Biopharma, Iovance, Jansen, Mallinckrodt, Merck, Mosaic ImmunoEngineering, Novartis, Oncosec, Pfizer, Targovax, and Teiko, and has received research funding from BMS and Incyte.
Z.E. Reports serving on advisory boards: Array, Pfizer, OncoSec, Regeneron, Genentech, Novartis, Natera; Research funding: Novartis, Pfizer, Boehringer-Ingelheim
S.C. reports serving on the Advisory Boards of Bristol Myers Squibb, Novartis, Pfizer and Regeneron.
E.M. reports no conflicts of interest.
C.R.G. reports no conflicts of interest.
I.B.C. reports no conflicts of interest.
A. V-C. Reports no relevant competing interests to disclose
I.P.G. Reports none.
E.S. Reports none.
S.H-L. reports the following: Consulting: Amgen, Genmab, Xencor, Regeneron, Nektar, Astellas, BMS, Merck; Research support: Amgen, Merck; Contracted Research: Pfizer, Plexxikon, Genentech, Neon Therapeutics, Nektar, Astellas, F Star, Xencor, Merck, Vedanta, Kite Pharma, Boehringer, Ingelheim, OncoC4, Dragonfly, BMS, BioAlta.
S.P.P. reports relevant competing interests: Bristol Myers-Squibb – clinical trial support (institution); advisory board; Cardinal Health – advisory board; Castle Biosciences – advisory board; Delcath - advisory board; consultant; Foghorn Therapeutics – clinical trial support (institution); Ideaya - clinical trial support (institution); Immunocore – data safety monitoring board; Immatics - advisory board; InxMed – clinical trial support (institution); Lyvgen Biopharma - clinical trial support (institution); Novartis – clinical trial support (institution); advisory board; consultant; Pfizer - advisory board; Provectus Biopharmaceuticals – clinical trial support; research support (institution); Reata Pharmaceuticals – clinical trial support (institution), data safety monitoring board; Replimmune - advisory board; TriSalus Life Sciences - scientific advisory board; clinical trial support (institution); Seagen - clinical trial support (institution); Syntrix Bio - clinical trial support (institution); Advance Knowledge in Healthcare – consulting.
K.F.G. is an employee and stockholder of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Newark, NJ, USA
S.L.B. reports none.
M.C.W. reports none.
A.R. has received honoraria from consulting with Amgen, Bristol-Myers Squibb and Merck, is or has been a member of the scientific advisory board and holds stock in Advaxis, Appia, Apricity, Arcus, Compugen, CytomX, Highlight, ImaginAb, ImmPact, ImmuneSensor, Inspirna, Isoplexis, Kite-Gilead, Lutris, MapKure, Merus, PACT, Pluto, RAPT, Synthekine and Tango, has received research funding from Agilent and from Bristol-Myers Squibb through Stand Up to Cancer (SU2C), and patent royalties from Arsenal Bio.
Figures
References
-
- Robert C, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med 372, 320–330 (2015). - PubMed
-
- Robert C, et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N Engl J Med 372, 2521–2532 (2015). - PubMed
-
- Ribas A, et al. Association of Pembrolizumab With Tumor Response and Survival Among Patients With Advanced Melanoma. JAMA 315, 1600–1609 (2016). - PubMed
