

Physiological effects of awake prone position in acute hypoxemic respiratory failure
- PMID: 37592288
- PMCID: PMC10433569
- DOI: 10.1186/s13054-023-04600-9
Physiological effects of awake prone position in acute hypoxemic respiratory failure
Abstract
Background: The effects of awake prone position on the breathing pattern of hypoxemic patients need to be better understood. We conducted a crossover trial to assess the physiological effects of awake prone position in patients with acute hypoxemic respiratory failure.
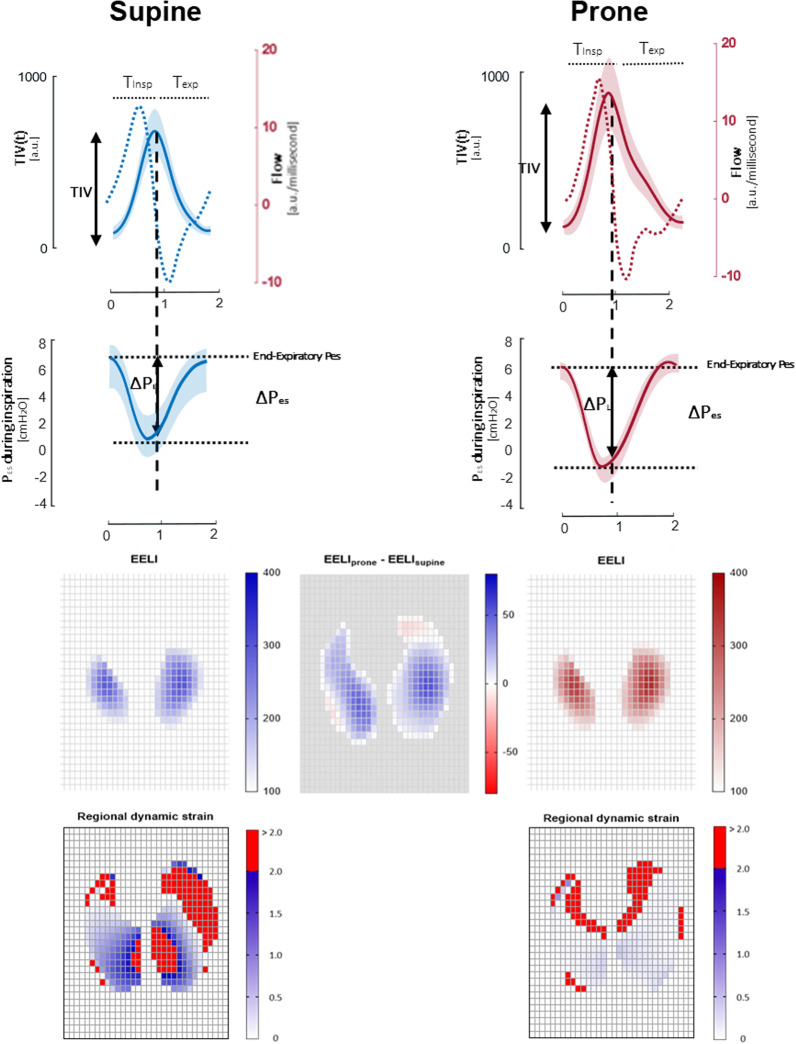
Methods: Fifteen patients with acute hypoxemic respiratory failure and PaO2/FiO2 < 200 mmHg underwent high-flow nasal oxygen for 1 h in supine position and 2 h in prone position, followed by a final 1-h supine phase. At the end of each study phase, the following parameters were measured: arterial blood gases, inspiratory effort (ΔPES), transpulmonary driving pressure (ΔPL), respiratory rate and esophageal pressure simplified pressure-time product per minute (sPTPES) by esophageal manometry, tidal volume (VT), end-expiratory lung impedance (EELI), lung compliance, airway resistance, time constant, dynamic strain (VT/EELI) and pendelluft extent through electrical impedance tomography.
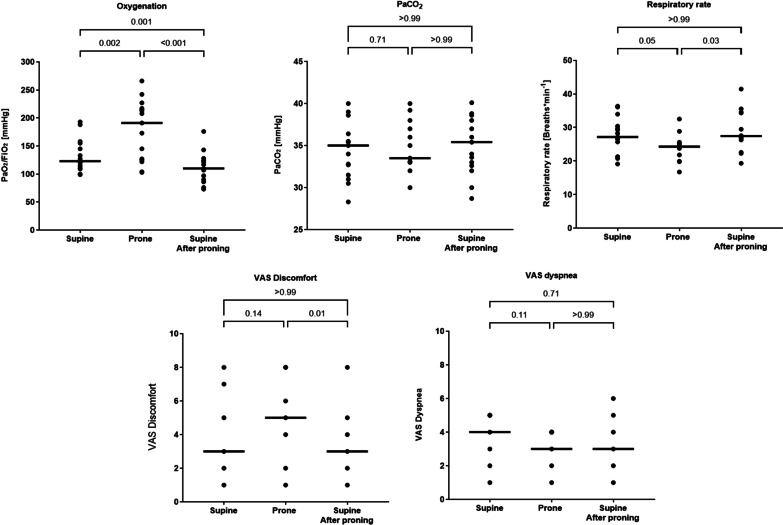
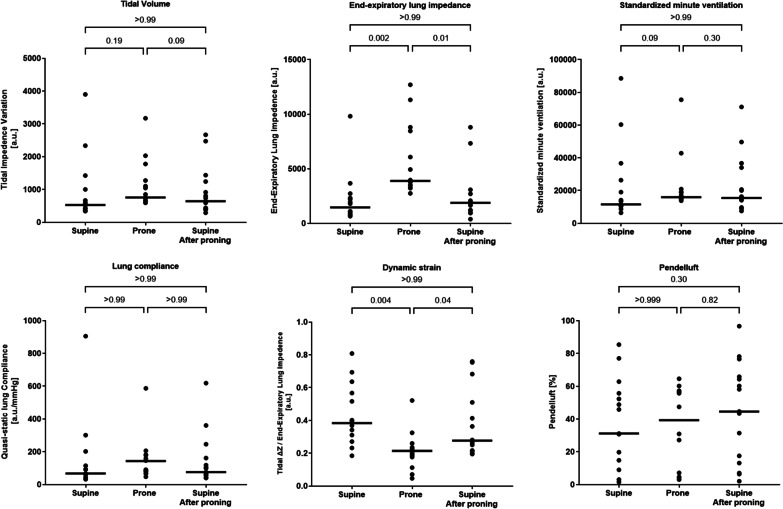
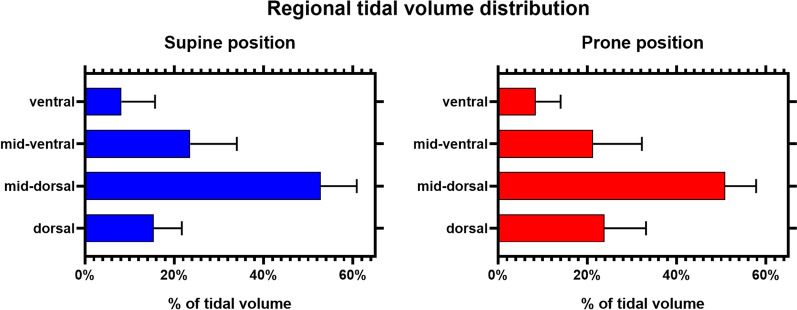
Results: Compared to supine position, prone position increased PaO2/FiO2 (median [Interquartile range] 104 mmHg [76-129] vs. 74 [69-93], p < 0.001), reduced respiratory rate (24 breaths/min [22-26] vs. 27 [26-30], p = 0.05) and increased ΔPES (12 cmH2O [11-13] vs. 9 [8-12], p = 0.04) with similar sPTPES (131 [75-154] cmH2O s min-1 vs. 105 [81-129], p > 0.99) and ΔPL (9 [7-11] cmH2O vs. 8 [5-9], p = 0.17). Airway resistance and time constant were higher in prone vs. supine position (9 cmH2O s arbitrary units-3 [4-11] vs. 6 [4-9], p = 0.05; 0.53 s [0.32-61] vs. 0.40 [0.37-0.44], p = 0.03). Prone position increased EELI (3887 arbitrary units [3414-8547] vs. 1456 [959-2420], p = 0.002) and promoted VT distribution towards dorsal lung regions without affecting VT size and lung compliance: this generated lower dynamic strain (0.21 [0.16-0.24] vs. 0.38 [0.30-0.49], p = 0.004). The magnitude of pendelluft phenomenon was not different between study phases (55% [7-57] of VT in prone vs. 31% [14-55] in supine position, p > 0.99).
Conclusions: Prone position improves oxygenation, increases EELI and promotes VT distribution towards dependent lung regions without affecting VT size, ΔPL, lung compliance and pendelluft magnitude. Prone position reduces respiratory rate and increases ΔPES because of positional increases in airway resistance and prolonged expiratory time. Because high ΔPES is the main mechanistic determinant of self-inflicted lung injury, caution may be needed in using awake prone position in patients exhibiting intense ΔPES. Clinical trail registeration: The study was registered on clinicaltrials.gov (NCT03095300) on March 29, 2017.
Keywords: Acute respiratory failure; Awake prone position; High-flow nasal oxygen; Inspiratory effort; Patient self-inflicted lung injury.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
DLG has received speaking fees by Gilead, Intersurgical, MSD and GE, and reports having received travel accommodation by Fisher and Paykel. MA has received personal fees by Maquet, and a research grant by Toray. DLG and MA disclose a research grant by GE.
Figures

References
-
- Gattinoni L, Carlesso E, Taccone P, Polli F, Guérin C, Mancebo J. Prone positioning improves survival in severe ARDS: a pathophysiologic review and individual patient meta-analysis. Miner Anestesiol. 2010;76:448–454. - PubMed
-
- Guerin C, Baboi L, Richard JC. Mechanisms of the effects of prone positioning in acute respiratory distress syndrome. Intensive Care Med. 2014;40:1634–1642. - PubMed
-
- Guérin C, Reignier J, Richard J-C, Beuret P, Gacouin A, Boulain T, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368:2159–2168. - PubMed
-
- Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195:1253–1263. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
