

Apoptosis inhibitor of macrophage (AIM)/CD5L is involved in the pathogenesis of COPD
- PMID: 37592330
- PMCID: PMC10433671
- DOI: 10.1186/s12931-023-02508-0
Apoptosis inhibitor of macrophage (AIM)/CD5L is involved in the pathogenesis of COPD
Abstract
Background: Alveolar macrophages (AMs) and AM-produced matrix metalloprotease (MMP)-12 are known to play critical roles in the pathogenesis of chronic obstructive pulmonary disease (COPD). The apoptosis inhibitor of the macrophages (AIM)/CD5 molecule-like (CD5L) is a multifunctional protein secreted by the macrophages that mainly exists in the blood in a combined form with the immunoglobulin (Ig)M pentamer. Although AIM has both facilitative and suppressive roles in various diseases, its role in COPD remains unclear.
Methods: We investigated the role of AIM in COPD pathogenesis using porcine pancreas elastase (PPE)-induced and cigarette smoke-induced emphysema mouse models and an in vitro model using AMs. We also analyzed the differences in the blood AIM/IgM ratio among nonsmokers, healthy smokers, and patients with COPD and investigated the association between the blood AIM/IgM ratio and COPD exacerbations and mortality in patients with COPD.
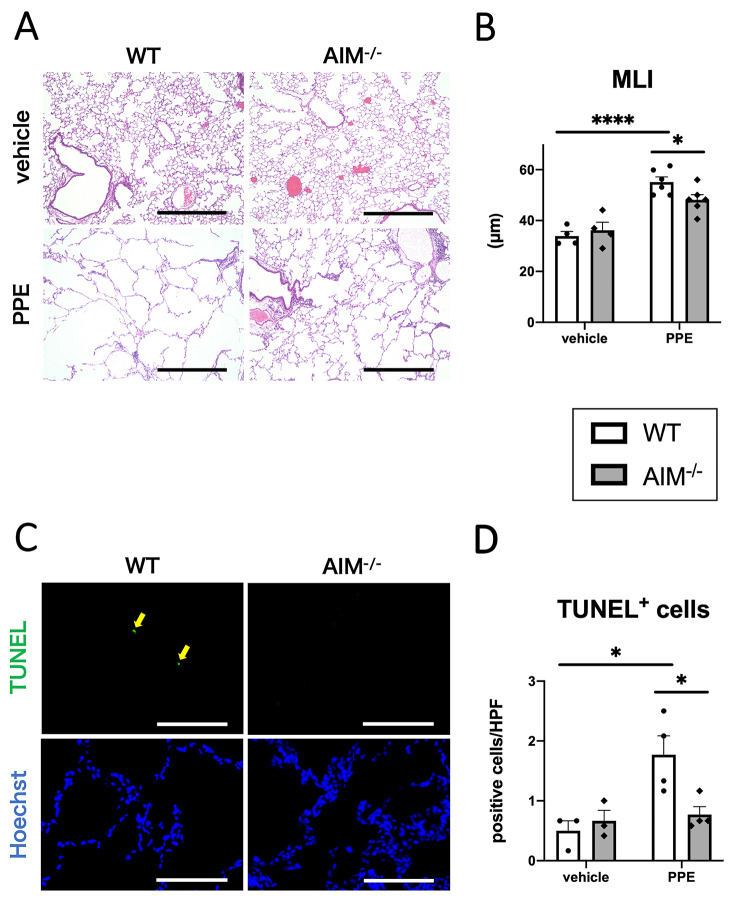
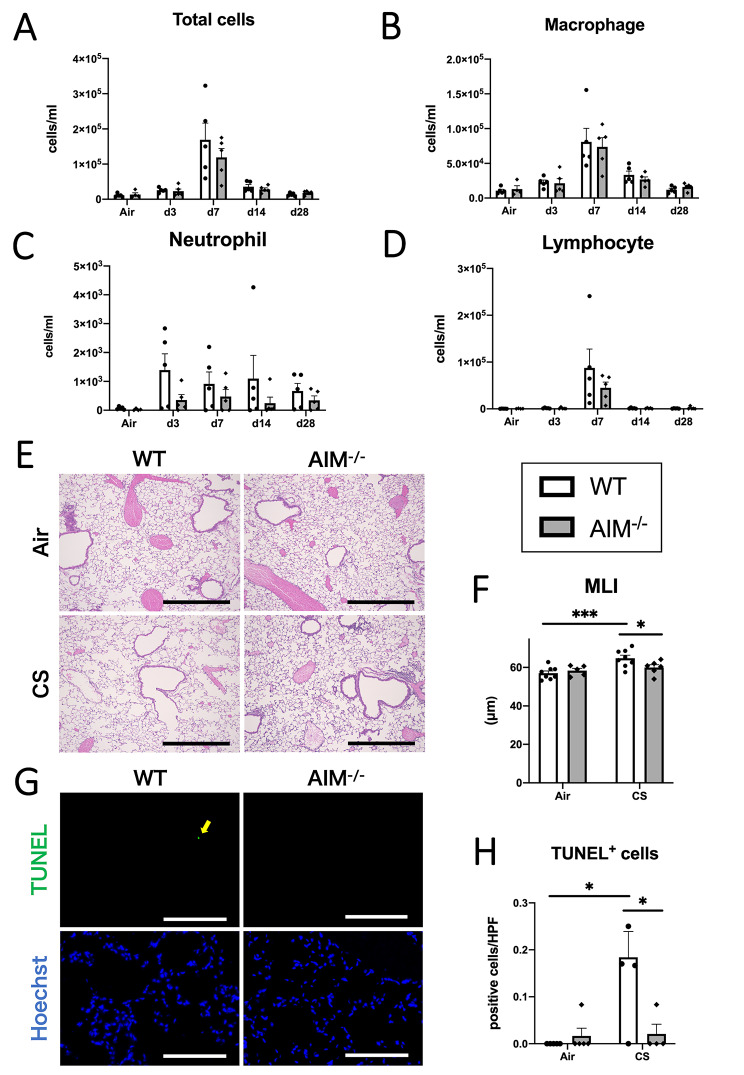
Results: Emphysema formation, inflammation, and cell death in the lungs were attenuated in AIM-/- mice compared with wild-type (WT) mice in both PPE- and cigarette smoke-induced emphysema models. The PPE-induced increase in MMP-12 was attenuated in AIM-/- mice at both the mRNA and protein levels. According to in vitro experiments using AMs stimulated with cigarette smoke extract, the MMP-12 level was decreased in AIM-/- mice compared with WT mice. This decrease was reversed by the addition of recombinant AIM. Furthermore, an analysis of clinical samples showed that patients with COPD had a higher blood AIM/IgM ratio than healthy smokers. Additionally, the blood AIM/IgM ratio was positively associated with disease severity in patients with COPD. A higher AIM/IgM ratio was also associated with a shorter time to the first COPD exacerbation and higher all-cause and respiratory mortality.
Conclusions: AIM facilitates the development of COPD by upregulating MMP-12. Additionally, a higher blood AIM/IgM ratio was associated with poor prognosis in patients with COPD.
Trial registration: This clinical study, which included nonsmokers, healthy smokers, and smokers with COPD, was approved by the Ethics Committee of the Hokkaido University Hospital (012-0075, date of registration: September 5, 2012). The Hokkaido COPD cohort study was approved by the Ethics Committee of the Hokkaido University School of Medicine (med02-001, date of registration: December 25, 2002).
Keywords: Alveolar macrophage; Apoptosis inhibitor of macrophage; Chronic obstructive lung disease; Matrix metalloprotease-12.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Pauwels RA, Rabe KF. Burden and clinical features of chronic obstructive pulmonary disease (COPD) Lancet. 2004;364(9434):613–20. - PubMed
-
- World Health Organization. : The top 10 causes of death. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death. Accessed on 7 March 2023.
-
- Barnes PJ. Alveolar macrophages as orchestrators of COPD. COPD. 2004;1(1):59–70. - PubMed
-
- Brusselle GG, Joos GF, Bracke KR. New insights into the immunology of chronic obstructive pulmonary disease. Lancet. 2011;378(9795):1015–26. - PubMed
-
- Hautamaki RD, Kobayashi DK, Senior RM, Shapiro SD. Requirement for macrophage elastase for cigarette smoke-induced emphysema in mice. Science. 1997;277(5334):2002–4. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
