

Differential effect on mortality of the timing of initiation of renal replacement therapy according to the criteria used to diagnose acute kidney injury: an IDEAL-ICU substudy
- PMID: 37592355
- PMCID: PMC10436583
- DOI: 10.1186/s13054-023-04602-7
Differential effect on mortality of the timing of initiation of renal replacement therapy according to the criteria used to diagnose acute kidney injury: an IDEAL-ICU substudy
Abstract
Background: This substudy of the randomized IDEAL-ICU trial assessed whether the timing of renal replacement therapy (RRT) initiation has a differential effect on 90-day mortality, according to the criteria used to diagnose acute kidney injury (AKI), in patients with early-stage septic shock.
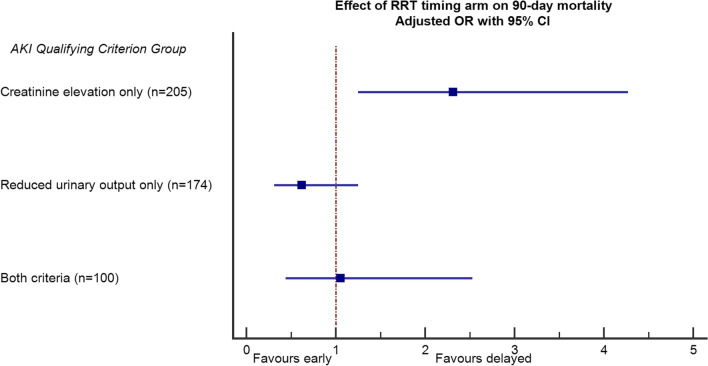
Methods: Three groups were considered according to the criterion defining AKI: creatinine elevation only (group 1), reduced urinary output only (group 2), creatinine elevation plus reduced urinary output (group 3). Primary outcome was 90-day all-cause death. Secondary endpoints were RRT-free days, RRT dependence and renal function at discharge. We assessed the interaction between RRT strategy (early vs. delayed) and group, and the association between RRT strategy and mortality in each group by logistic regression.
Results: Of 488 patients enrolled, 205 (42%) patients were in group 1, 174 (35%) in group 2, and 100 (20%) in group 3. The effect of RRT initiation strategy on 90-day mortality across groups showed significant heterogeneity (adjusted interaction p = 0.021). Mortality was 58% vs. 42% for early vs. late RRT initiation, respectively, in group 1 (p = 0.028); 57% vs. 67%, respectively, in group 2 (p = 0.18); and 58% vs. 55%, respectively, in group 3 (p = 0.79). There was no significant difference in secondary outcomes.
Conclusion: The timing of RRT initiation has a differential impact on outcome according to AKI diagnostic criteria. In patients with elevated creatinine only, early RRT initiation was associated with significantly increased mortality. In patients with reduced urine output only, late RRT initiation was associated with a nonsignificant, 10% absolute increase in mortality.
Keywords: Intensive care unit; Kidney failure; Renal replacement therapy; Septic shock.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
No author has any conflict of interest to declare.
Figures
References
-
- Investigators S-A, Canadian Critical Care Trials G, Australian, New Zealand Intensive Care Society Clinical Trials G, United Kingdom Critical Care Research G, Canadian Nephrology Trials N et al. Timing of initiation of renal-replacement therapy in acute kidney injury. N Engl J Med 2020, 383:240–251. 10.1056/NEJMoa2000741
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
