

Atrial fibrillation ablation in patients with arrhythmia-induced cardiomyopathy: a prospective multicentre study
- PMID: 37593841
- PMCID: PMC10567669
- DOI: 10.1002/ehf2.14448
Atrial fibrillation ablation in patients with arrhythmia-induced cardiomyopathy: a prospective multicentre study
Abstract
Aims: This study aims to investigate the clinical and biochemical characteristics of patients with atrial fibrillation (AF) referred for ablation who develop arrhythmia-induced cardiomyopathy (AiCM) as well as their long-term outcomes after catheter ablation (CA).
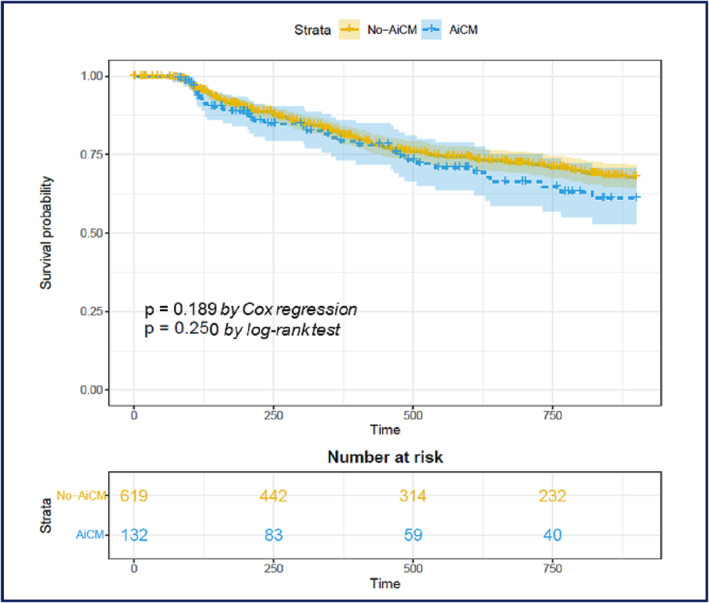
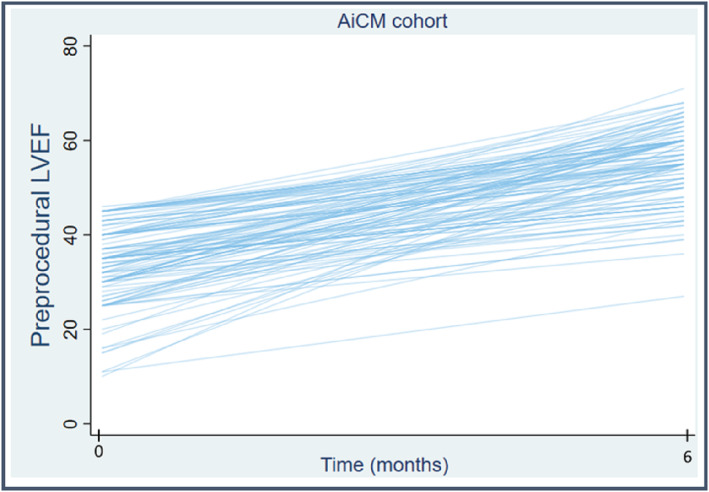
Methods and results: A prospective multicentre study was conducted on consecutive AF patients who underwent CA. AiCM was defined as the development of heart failure in the presence of AF and an improvement of left ventricular fraction by at least 10% at 6 months after ablation. A subgroup of patients underwent peripheral and left atrial blood samples [galectin-3, fatty acid-binding protein 4 (FABP4), and soluble receptor for advanced glycation end products (sRAGE)] at the time of the procedure. Of the 769 patients who underwent AF ablation, 135 (17.56%) met the criteria for AiCM. Independent predictors of AiCM included persistent AF, male gender, left atrial volume, QRS width, active smoking, and chronic kidney disease (CKD). Biomarker analysis revealed that sRAGE, FABP4, and galectin-3 levels were not predictive of AiCM development nor did they differ between groups or predict recurrence. There were no differences in AF recurrence between patients with and without AiCM (30.83% vs. 27.77%; P = 0.392) during a median follow-up of 23.83 months (inter-quartile range 9-36).
Conclusions: In the subset of patients referred for AF ablation, the development of AiCM was associated with persistent AF and CKD. Biomarker analysis was not different between groups nor predicted recurrence. Patients with AiCM benefited from ablation, with a significant improvement in left ventricular ejection fraction and similar AF recurrence rates to those without AiCM.
Keywords: Atrial fibrillation; Catheter ablation; Heart failure.
© 2023 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures

References
-
- Watanabe H, Okamura K, Chinushi M, Chinushi M, Furushima H, Tanabe Y, Kodama M, Aizawa Y. Clinical characteristics, treatment, and outcome of tachycardia induced cardiomyopathy. Int Heart J. 2008; 49: 39–47. - PubMed
-
- Redfield MM, Kay GN, Jenkins LS, Mianulli M, Jensen DN, Ellenbogen KA, APT investigators . Tachycardia‐related cardiomyopathy: a common cause of ventricular dysfunction in patients with atrial fibrillation referred for atrioventricular ablation. Mayo Clin Proc. 2000; 75: 790–795. - PubMed
-
- Gentlesk PJ, Sauer WH, Gerstenfeld EP, Lin D, Dixit S, PA‐C EZ, Callans D, Marchlinski FE. Reversal of left ventricular dysfunction following ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2007; 18: 9–14. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous