

Impact on the Volume of Pathology Reports Before and During the COVID-19 Pandemic in SEER Cancer Registries
- PMID: 37594474
- PMCID: PMC10618747
- DOI: 10.1158/1055-9965.EPI-23-0066
Impact on the Volume of Pathology Reports Before and During the COVID-19 Pandemic in SEER Cancer Registries
Abstract
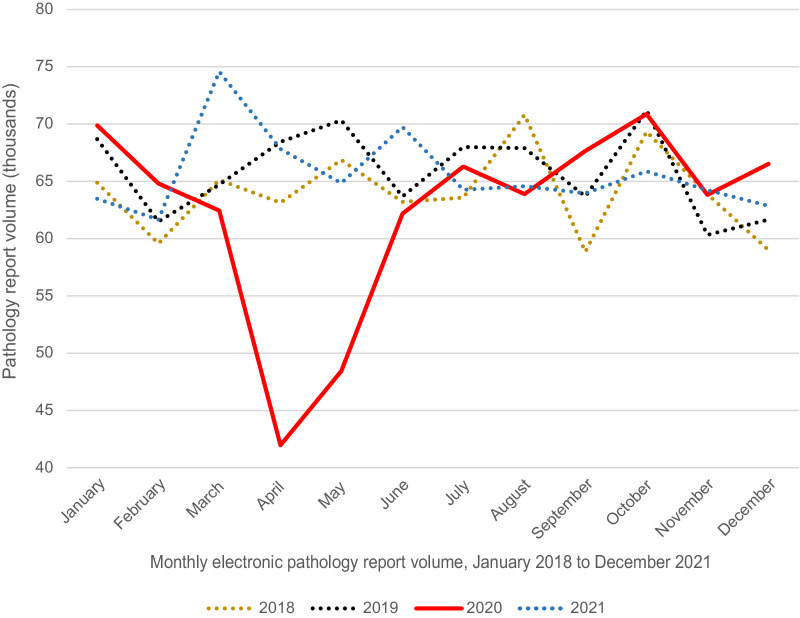
Introduction: Health care procedures including cancer screening and diagnosis were interrupted due to the COVID-19 pandemic. The extent of this impact on cancer care in the United States is not fully understood. We investigated pathology report volume as a reflection of trends in oncology services pre-pandemic and during the pandemic.
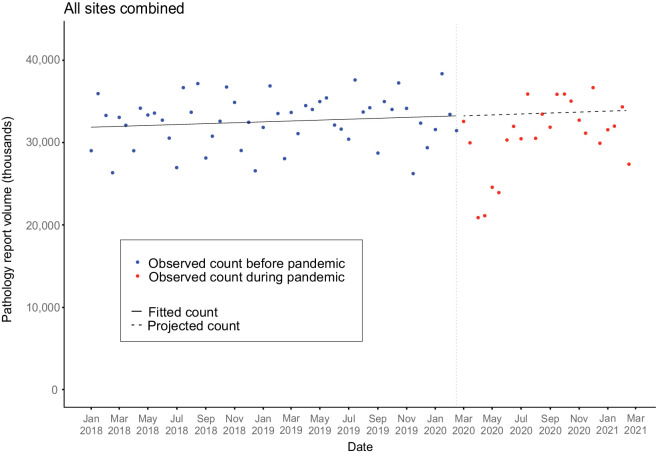
Methods: Electronic pathology reports were obtained from 11 U.S. central cancer registries from NCI's SEER Program. The reports were sorted by cancer site and document type using a validated algorithm. Joinpoint regression was used to model temporal trends from January 2018 to February 2020, project expected counts from March 2020 to February 2021 and calculate observed-to-expected ratios. Results were stratified by sex, age, cancer site, and report type.
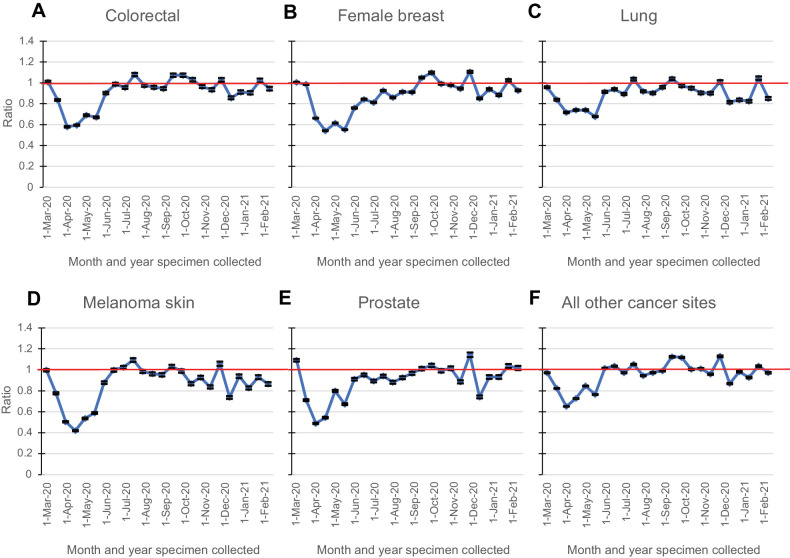
Results: During the first 3 months of the pandemic, pathology report volume decreased by 25.5% and 17.4% for biopsy and surgery reports, respectively. The 12-month O/E ratio (March 2020-February 2021) was lowest for women (O/E 0.90) and patients 65 years and older (O/E 0.91) and lower for cancers with screening (melanoma skin, O/E 0.86; breast, O/E 0.88; lung O/E 0.89, prostate, O/E 0.90; colorectal, O/E 0.91) when compared with all other cancers combined.
Conclusions: These findings indicate a decrease in cancer diagnosis, likely due to the COVID-19 pandemic. This decrease in the number of pathology reports may result in a stage shift causing a subsequent longer-term impact on survival patterns.
Impact: Investigation on the longer-term impact of the pandemic on pathology services is vital to understand if cancer care delivery levels continue to be affected.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Centers for Disease Control and Prevention. CDC museum COVID-19 timeline. 2022. [cited 2022 Nov 7]. Available from: https://www.cdc.gov/museum/timeline/covid19.html.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
