

Minimally invasive plate osteosynthesis (MIPO) for scapular fractures
- PMID: 37594566
- PMCID: PMC10697868
- DOI: 10.1007/s00064-023-00819-5
Minimally invasive plate osteosynthesis (MIPO) for scapular fractures
Abstract
Objective: Presentation of a minimally invasive surgical approach for the treatment of scapular fractures and the clinical outcome using this technique.
Indications: Displaced extra-articular fractures of the scapula body and glenoid neck (AO 14B and 14F) and simple intra-articular fractures of the glenoid.
Contraindications: Complex intra-articular fractures and isolated fractures of the coracoid base.
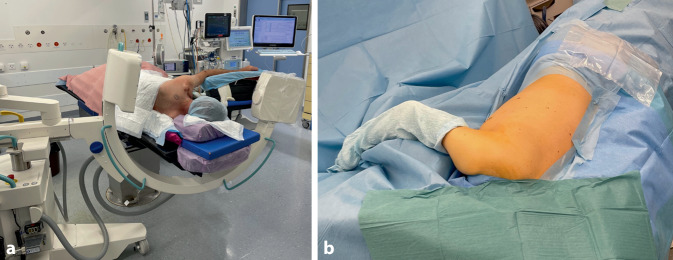
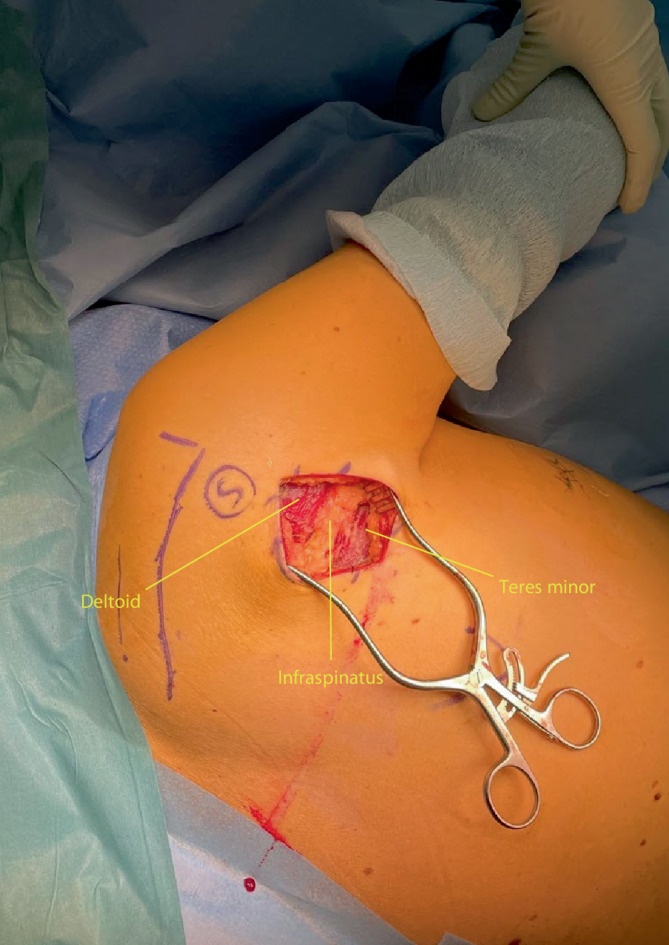
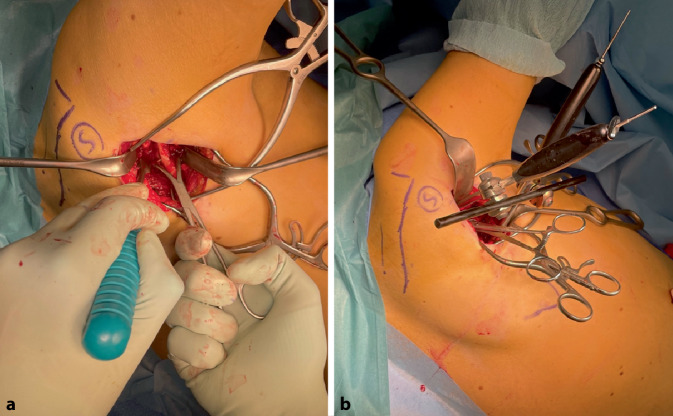
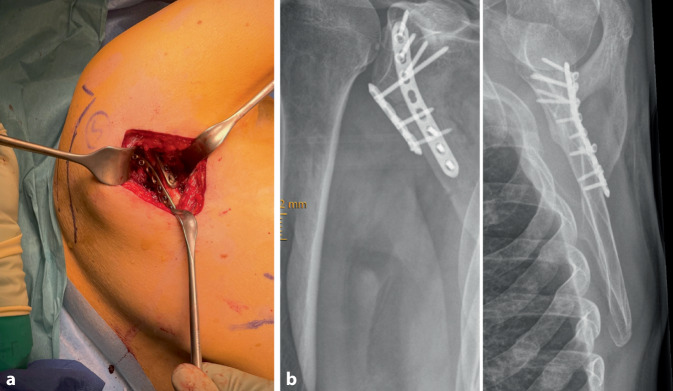
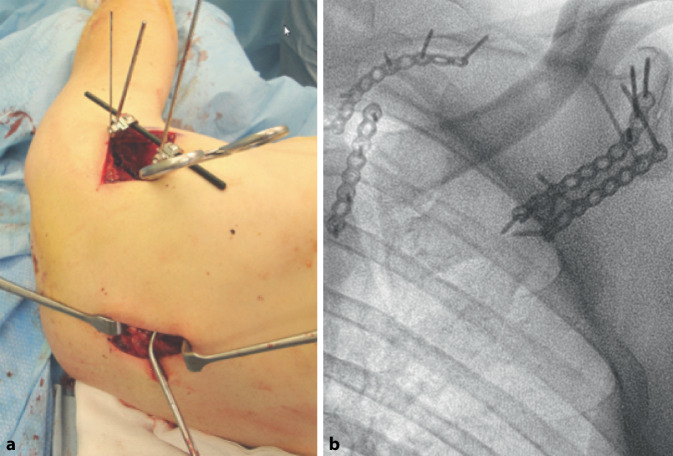
Surgical technique: Make a straight or slightly curved incision along the lateral margin of the scapula leaving the deltoid fascia intact. Identify the interval between the teres minor muscle and infraspinatus to visualize the lateral column, whilst retracting the deltoid to visualize the glenoid neck. Reduce and align the fracture using direct and indirect reduction tools. A second window on the medial border of the scapula can be made to aid reduction and/or to augment stability. Small (2.0-2.7 mm) plates in a 90° configuration on the lateral border and, if required, on the medial border are used. Intra-operative imaging confirms adequate reduction and extra-articular screw placement.
Postoperative management: Direct postoperative free functional nonweight-bearing rehabilitation limited to 90° abduction for the first 6 weeks. Sling for comfort. Free range of motion and permissive weight-bearing after 6 weeks.
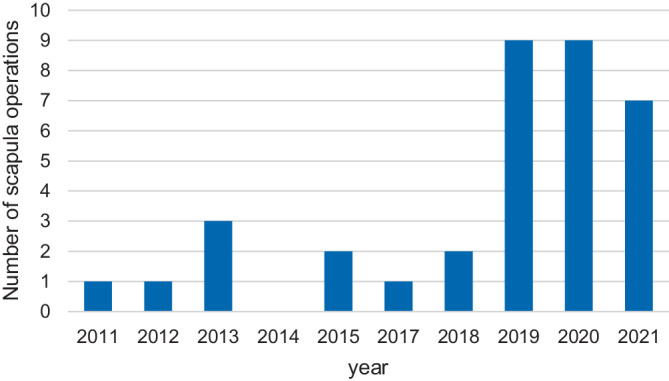
Results: We collected data from 35 patients treated with minimally invasive plate osteosynthesis (MIPO) between 2011 and 2021. Average age was 53 ± 15.1 years (range 21-71 years); 17 had a type B and 18 a type F fracture according the AO classification. All patients suffered concomitant injuries of which thoracic (n = 33) and upper extremity (n = 25) injuries were most common. Double plating of the lateral border (n = 30) was most commonly performed as described in the surgical technique section. One patient underwent an additional osteosynthesis 3 months after initial surgery due to pain and lack of radiological signs of healing of a fracture extension into the spine of the scapula. In the same patient, the plate on the spine of scapula was later removed due to plate irritation. In 2 patients postoperative images showed a screw protruding into the glenohumeral joint requiring revision surgery. After standardisation of intra-operative imaging following these two cases, intra-articular screw placement did not occur anymore. No patient suffered from iatrogenic nerve injury and none developed a wound infection.
Zusammenfassung: OPERATIONSZIEL: Präsentation des minimal-invasiven Zugangs zur Versorgung von Skapulafrakturen samt klinischem Ausgang.
Indikationen: Dislozierte, extraartikuläre Frakturen des Skapulablatts sowie des Collum scapulae (AO 148 und 14F) sowie einfache intraartikuläre Frakturen des Glenoids.
Kontraindikationen: Komplexe intraartikuläre Frakturen und isolierte Frakturen der Basis des Processus coracoideus.
Operationstechnik: Setzen einer geraden oder leicht gebogenen Inzision entlang des lateralen Rands der Skapula unter Intaktlassen der Deltafaszie. Identifikation des Intervalls zwischen M. teres minor und M. infraspinatus zur Visualisierung des lateralen Skapulablatts. Der Deltamuskel wird dabei nach kranial weggehalten, um den Skapulahals zu visualisieren. Frakturreposition unter Verwendung von direkten und indirekten Repositionsinstrumenten. Ein zweites Fenster über der Facies medialis der Skapula kann dabei zur besseren Visualisierung oder Stabilisierung eröffnet werden. Verwendung kleiner (2,0–2,7 mm), im 90°-Winkel zueinander angeordneter Platten entlang der lateralen Begrenzung der Skapula oder – sofern nötig – medialseitig. Die intraoperative Kontrolle mittels Bildwandler bestätigt die korrekte Reposition und Lage des Osteosynthesematerials.
Weiterbehandlung: Sofortige postoperative funktionelle Behandlung ohne Belastung bis zur Horizontalen während der ersten 6 Wochen. Armschlinge zum Komfort. Nach 6 Wochen freie Beweglichkeit und Belastung.
Ergebnisse: Zwischen 2011 und 2021 behandelten wir 35 Patienten mit der MIPO(minimal-invasive Plattenosteosynthese)-Technik, welche im Mittel über 8 Monate (Bandbreite von 3 bis 31 Monate) nachbehandelt wurden. Das Durchschnittsalter belief sich auf 53 ± 15,1 Jahre (Bandbreite 21 bis 71); 17 Patienten wiesen eine B‑Fraktur, 18 eine F‑Fraktur nach AO(Arbeitsgemeinschaft für Osteosynthesefragen)-Klassifikation auf. In der Mehrzahl der Fälle (n = 30) erfolgte eine laterale Doppelplattenosteosynthese wie unter der Rubrik Operationstechnik beschrieben. Ein Patient wurde 3 Monate nach initialer Osteosynthese erneut operiert aufgrund von Schmerzen und fehlender radiologischer Konsolidation eines Frakturausläufers in die Spina scapulae. Die daraufhin eingebrachte Platte auf der Spina wurde später aufgrund von störendem Osteosynthesematerial wieder entfernt. Bei 2 Patienten erfolgte eine Revision aufgrund einer intraartikulär im Glenohumeralgelenk liegenden Schraube. Keiner der Patienten zeigte iatrogene Nervenläsionen oder Wundinfekte.
Keywords: Deltoid sparing; MIPO; Minimally invasive surgical procedures; Scapula fracture.
© 2023. The Author(s).
Conflict of interest statement
B.J.M. van de Wall, R.J. Hoepelman, C. Michelitsch, N. Diwersi, C. Sommer, R. Babst and F.J.P. Beeres declare that they have no competing interests.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
