

Transient loss and recovery of oral chemesthesis, taste and smell with COVID-19: A small case-control series
- PMID: 37595820
- PMCID: PMC10591985
- DOI: 10.1016/j.physbeh.2023.114331
Transient loss and recovery of oral chemesthesis, taste and smell with COVID-19: A small case-control series
Abstract
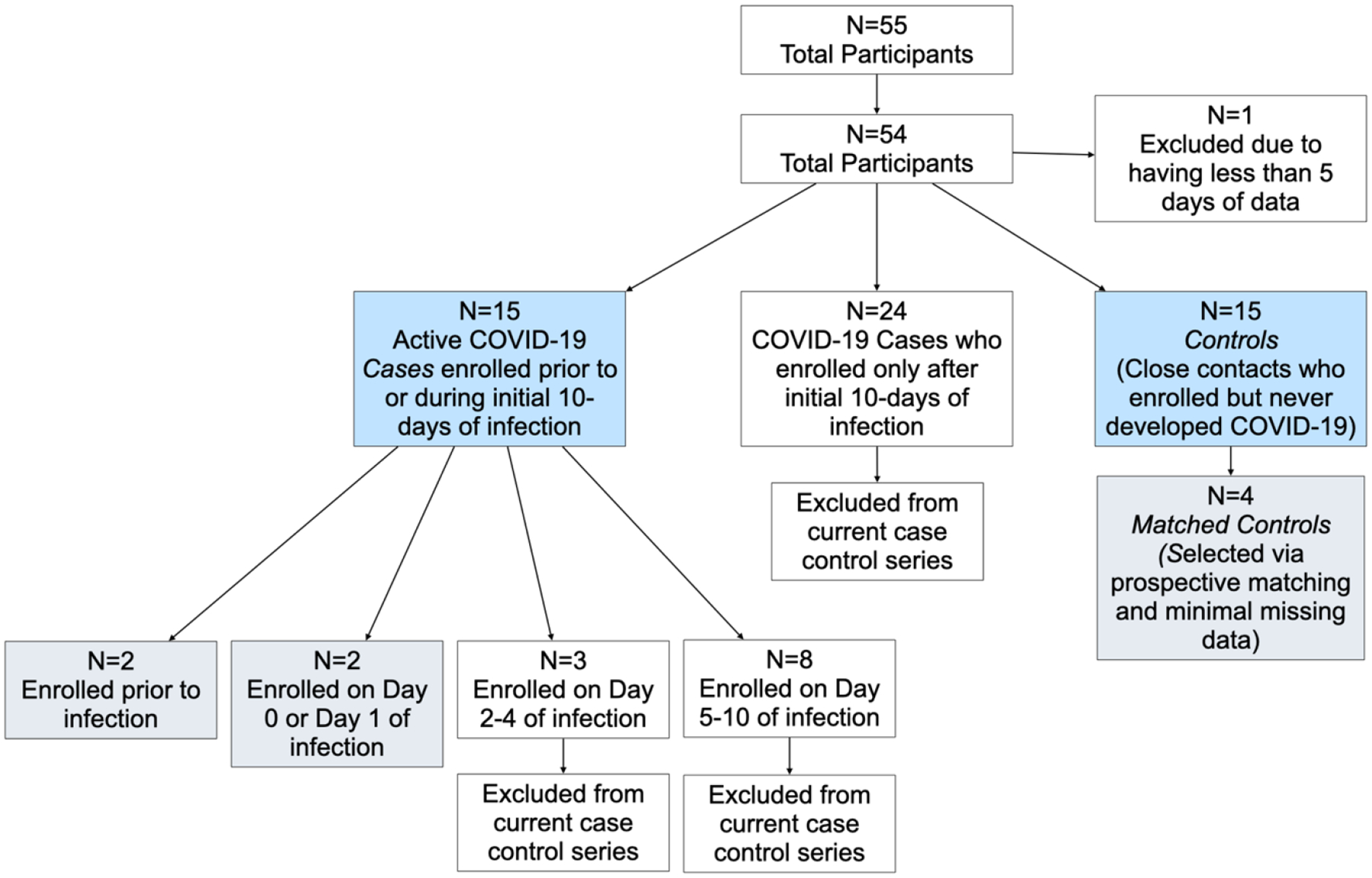
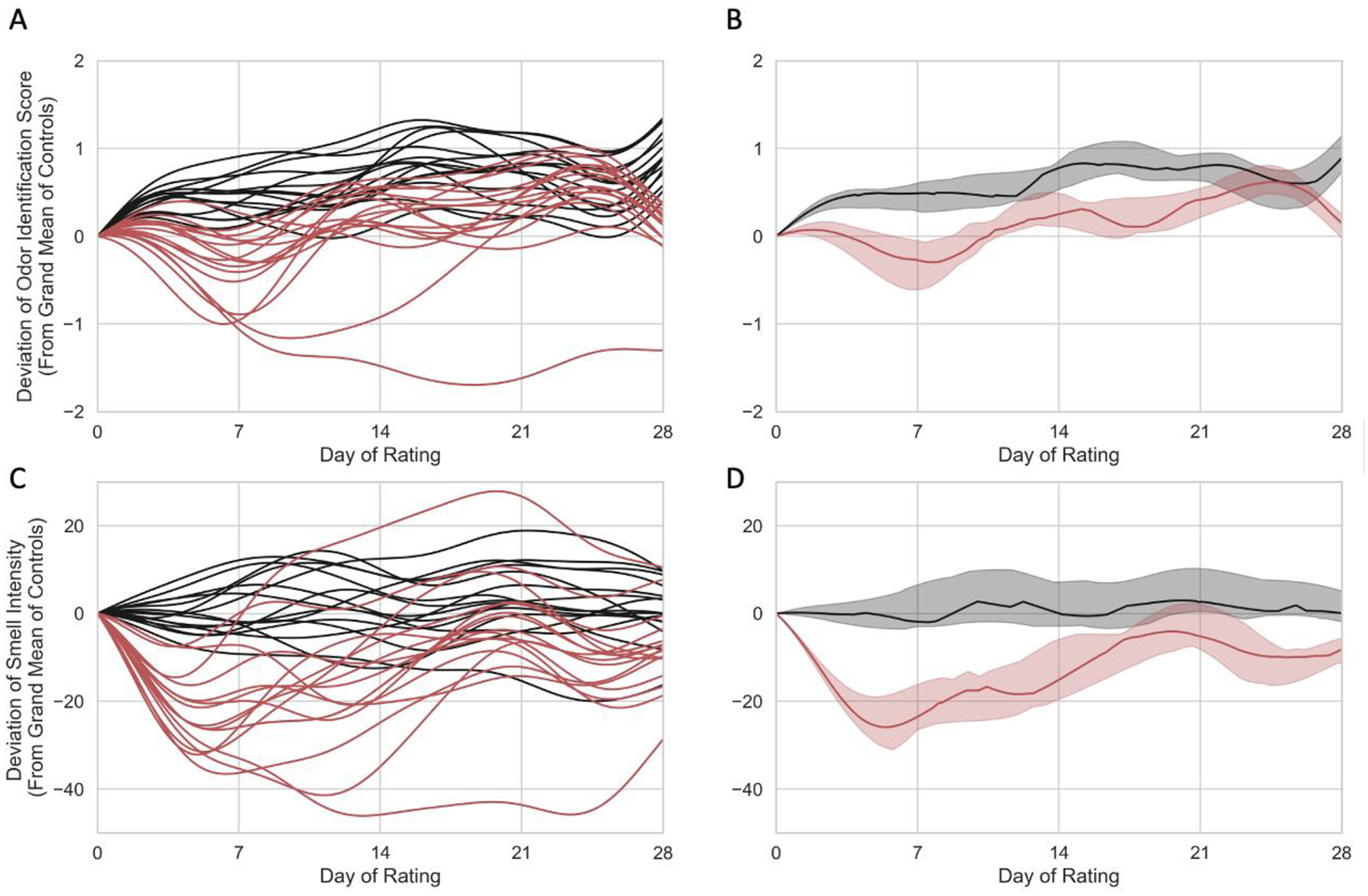
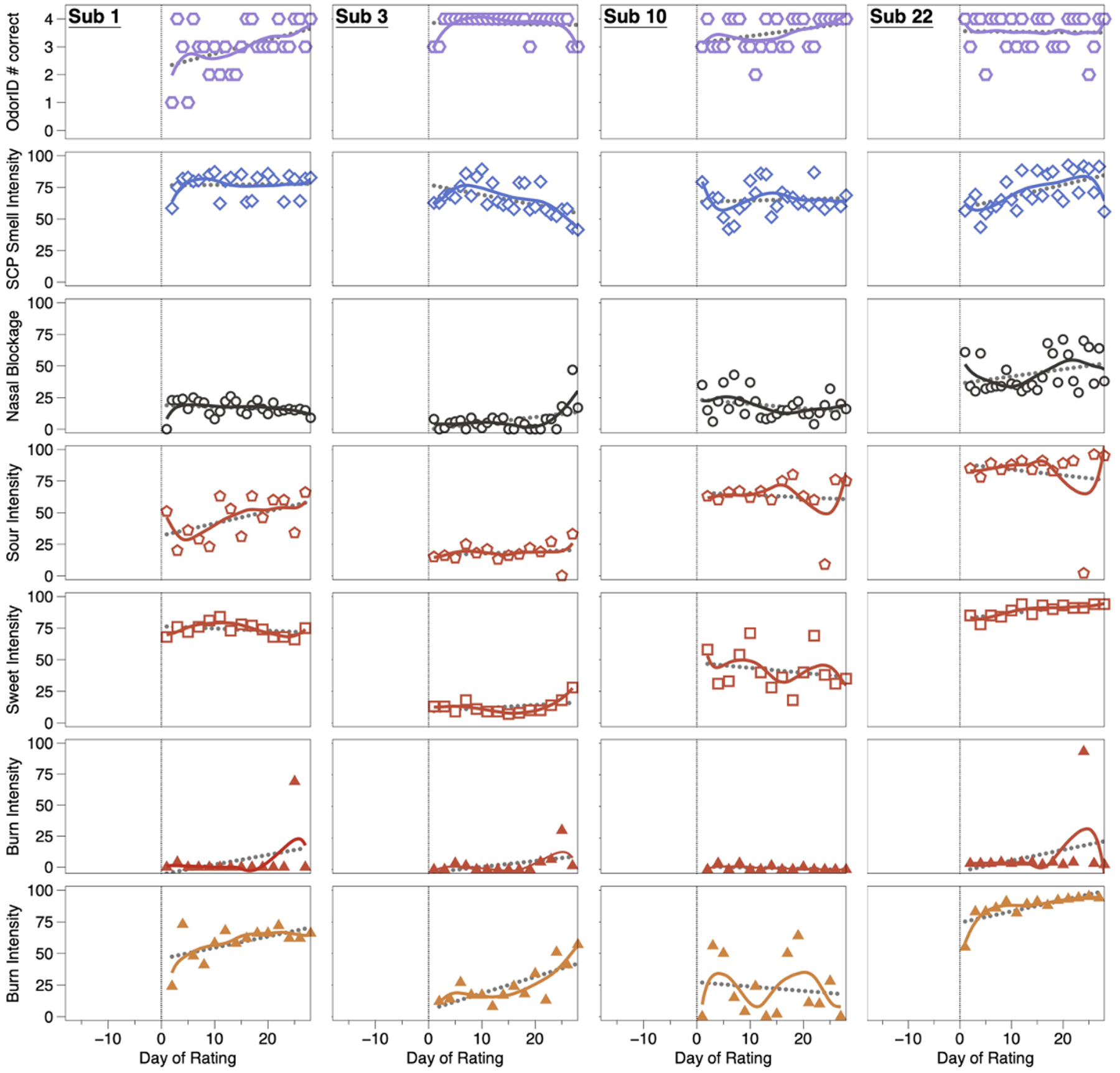
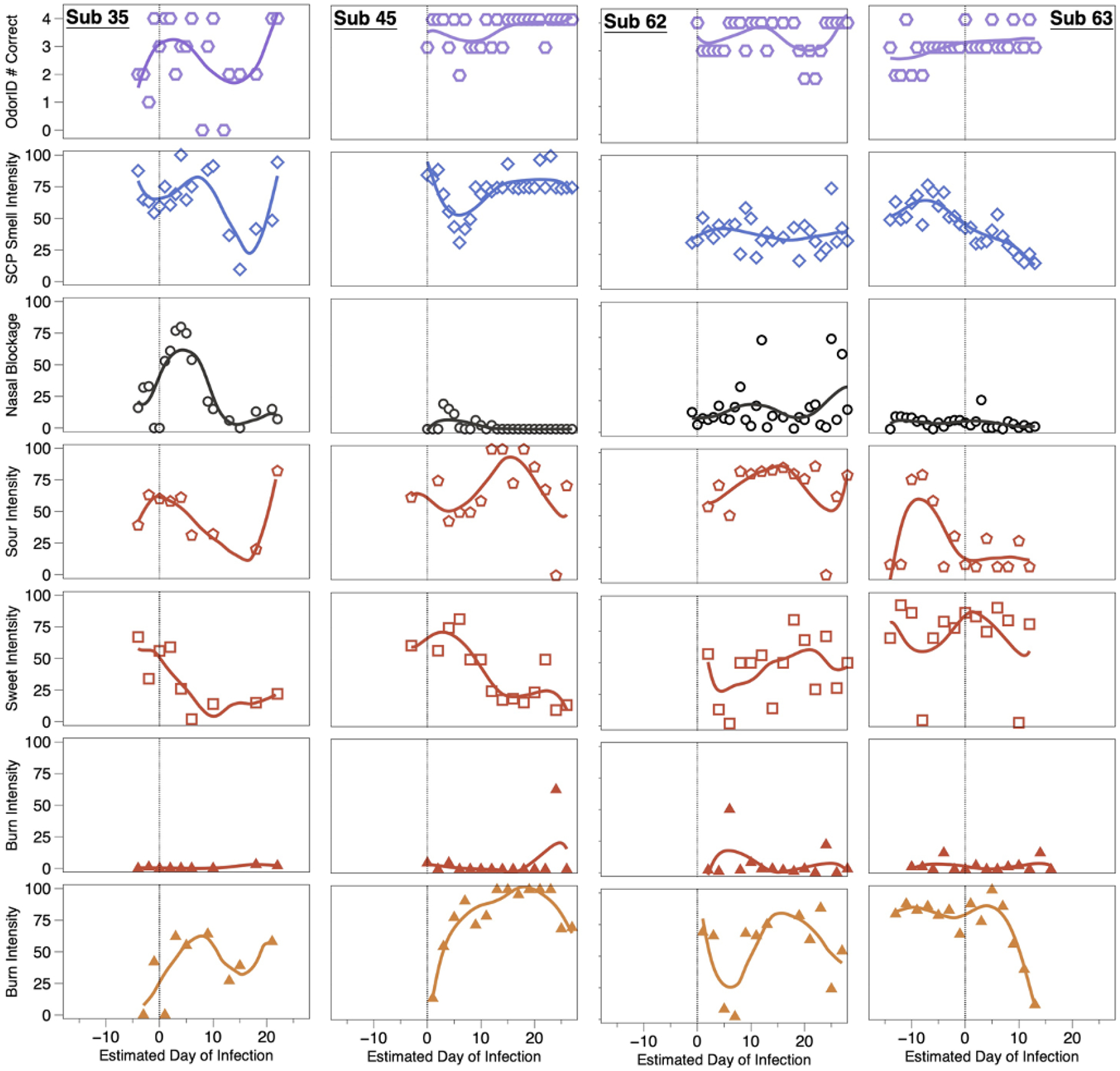
Transient loss of smell is a common symptom of influenza and other upper respiratory infections. Loss of taste is possible but rare with these illnesses, and patient reports of 'taste loss' typically arise from a taste / flavor confusion. Thus, initial reports from COVID-19 patients of loss of taste and chemesthesis (i.e., chemical somatosensation like warming or cooling) were met with skepticism until multiple studies confirmed SARS-CoV-2 infections could disrupt these senses. Many studies have been based on self-report or on single time point assessments after acute illness was ended. Here, we describe intensive longitudinal data over 28 days from adults aged 18-45 years recruited in early 2021 (i.e., prior to the Delta and Omicron SARS-CoV-2 waves). These individuals were either COVID-19 positive or close contacts (per U.S. CDC criteria at the time of the study) in the first half of 2021. Upon enrollment, all participants were given nose clips, blinded samples of commercial jellybeans (Sour Cherry and Cinnamon), and scratch-n-sniff odor identification test cards (ScentCheckPro), which they used for daily assessments. In COVID-19 cases who enrolled on or before Day 10 of infection, Gaussian Process Regression showed two distinct measures of function - odor identification and odor intensity - declined relative to controls (exposed individuals who never developed COVID-19). Because enrollment began upon exposure, some participants became ill only after enrollment, which allowed us to capture baseline ratings, onset of loss, and recovery. Data from these four cases and four age- and sex- matched controls were plotted over 28 days to create panel plots. Variables included mean orthonasal intensity of four odors (ScentCheckPro), perceived nasal blockage, oral burn (Cinnamon jellybeans), and sourness and sweetness (Sour Cherry jellybeans). Controls exhibited stable ratings over time. By contrast, COVID-19 cases showed sharp deviations over time. Changes in odor intensity or odor identification were not explained by nasal blockage. No single pattern of taste loss or recovery was apparent, implying different taste qualities might recover at different rates. Oral burn was transiently reduced for some before recovering quickly, suggesting acute loss may be missed in datasets collected only after illness ends. Collectively, intensive daily testing shows orthonasal smell, oral chemesthesis and taste were each altered by acute SARS-CoV-2 infection. This disruption was dyssynchronous for different modalities, with variable loss and recovery rates across both modalities and individuals.
Keywords: Anosmia; Gustation; Longitudinal; Olfaction; Recovery; Trigeminal.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest SDM, JEH, and RCG each hold equity in Redolynt, LLC, which they co-founded in 2021. This financial interest has been reviewed by the Individual Conflict of Interest Committee at each of their respective universities and is being actively managed by each university. None of the other authors have any conflicts to disclose.
Figures
Update of
-
Transient loss and recovery of oral chemesthesis, taste and smell with COVID-19: a small case-control series.medRxiv [Preprint]. 2023 Mar 29:2023.03.27.23287763. doi: 10.1101/2023.03.27.23287763. medRxiv. 2023. Update in: Physiol Behav. 2023 Nov 1;271:114331. doi: 10.1016/j.physbeh.2023.114331. PMID: 37034638 Free PMC article. Updated. Preprint.
Similar articles
-
Transient loss and recovery of oral chemesthesis, taste and smell with COVID-19: a small case-control series.medRxiv [Preprint]. 2023 Mar 29:2023.03.27.23287763. doi: 10.1101/2023.03.27.23287763. medRxiv. 2023. Update in: Physiol Behav. 2023 Nov 1;271:114331. doi: 10.1016/j.physbeh.2023.114331. PMID: 37034638 Free PMC article. Updated. Preprint.
-
More Than Smell-COVID-19 Is Associated With Severe Impairment of Smell, Taste, and Chemesthesis.Chem Senses. 2020 Oct 9;45(7):609-622. doi: 10.1093/chemse/bjaa041. Chem Senses. 2020. PMID: 32564071 Free PMC article.
-
Self-reported symptom study of COVID-19 chemosensory dysfunction in Malaysia.Sci Rep. 2022 Feb 8;12(1):2111. doi: 10.1038/s41598-022-06029-6. Sci Rep. 2022. PMID: 35136124 Free PMC article. Clinical Trial.
-
Olfactory and Gustatory Recovery Time Evaluation of COVID-19: A Systematic Review and Meta-Analysis.Acta Med Indones. 2025 Jan;57(1):18-43. Acta Med Indones. 2025. PMID: 40263685
-
Chemosensory loss in COVID-19.Oral Dis. 2022 Nov;28 Suppl 2:2337-2346. doi: 10.1111/odi.14300. Epub 2022 Jul 14. Oral Dis. 2022. PMID: 35790059 Free PMC article. Review.
Cited by
-
Living and Coping with Olfactory and Taste Disorders: A Qualitative Study of People with Long-COVID-19.Healthcare (Basel). 2024 Mar 30;12(7):754. doi: 10.3390/healthcare12070754. Healthcare (Basel). 2024. PMID: 38610176 Free PMC article.
References
-
- WHO. World Health Organization (COVID-19) Dashboard. 2022; Available from: https://covid19.who.int.
-
- Passarelli PC, Lopez MA, Bonaviri GM, Garcia-Godoy F, and D’Addona A, Taste and smell as chemosensory dysfunctions in COVID-19 infection. Am J Dent, 2020. 33(3): p. 135–137. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
