

Incretins and microvascular complications of diabetes: neuropathy, nephropathy, retinopathy and microangiopathy
- PMID: 37597048
- PMCID: PMC10474214
- DOI: 10.1007/s00125-023-05988-3
Incretins and microvascular complications of diabetes: neuropathy, nephropathy, retinopathy and microangiopathy
Abstract
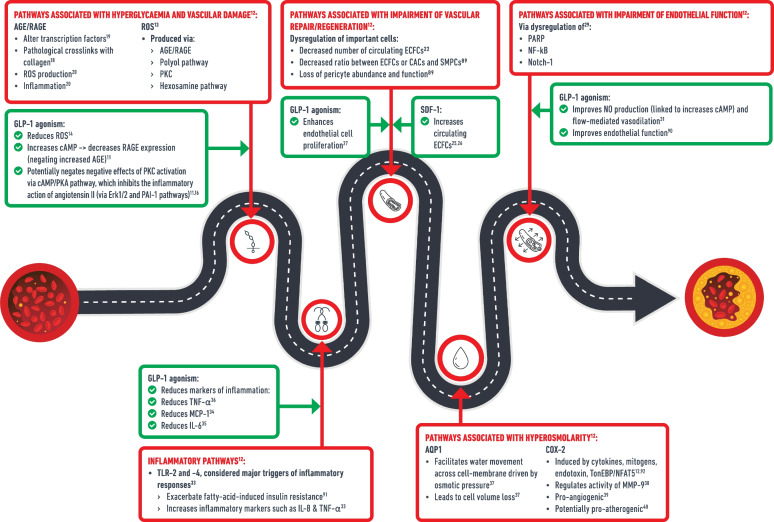
Glucagon-like peptide-1 receptor agonists (GLP-1RAs, incretin mimetics) and dipeptidyl peptidase-4 inhibitors (DPP-4is, incretin enhancers) are glucose-lowering therapies with proven cardiovascular safety, but their effect on microvascular disease is not fully understood. Both therapies increase GLP-1 receptor agonism, which is associated with attenuation of numerous pathological processes that may lead to microvascular benefits, including decreased reactive oxygen species (ROS) production, decreased inflammation and improved vascular function. DPP-4is also increase stromal cell-derived factor-1 (SDF-1), which is associated with neovascularisation and tissue repair. Rodent studies demonstrate several benefits of these agents in the prevention or reversal of nephropathy, retinopathy and neuropathy, but evidence from human populations is less clear. For nephropathy risk in human clinical trials, meta-analyses demonstrate that GLP-1RAs reduce the risk of a composite renal outcome (doubling of serum creatinine, eGFR reduction of 30%, end-stage renal disease or renal death), whereas the benefits of DPP-4is appear to be limited to reductions in the risk of albuminuria. The relationship between GLP-1RAs and retinopathy is less clear. Many large trials and meta-analyses show no effect, but an observed increase in the risk of retinopathy complications with semaglutide therapy (a GLP-1RA) in the SUSTAIN-6 trial warrants caution, particularly in individuals with baseline retinopathy. Similarly, DPP-4is are associated with increased retinopathy risk in both trials and meta-analysis. The association between GLP-1RAs and peripheral neuropathy is unclear due to little trial evidence. For DPP-4is, one trial and several observational studies show a reduced risk of peripheral neuropathy, with others reporting no effect. Evidence in other less-established microvascular outcomes, such as microvascular angina, cerebral small vessel disease, skeletal muscle microvascular disease and autonomic neuropathies (e.g. cardiac autonomic neuropathy, gastroparesis, erectile dysfunction), is sparse. In conclusion, GLP-1RAs are protective against nephropathy, whereas DPP-4is are protective against albuminuria and potentially peripheral neuropathy. Caution is advised with DPP-4is and semaglutide, particularly for patients with background retinopathy, due to increased risk of retinopathy. Well-designed trials powered for microvascular outcomes are needed to clarify associations of incretin therapies and microvascular diseases.
Keywords: DPP-4 inhibitors; GLP-1; GLP-1 receptor agonists; Incretin; Mechanisms; Microvascular disease; Nephropathy; Neuropathy; Pathophysiology; Retinopathy; Review; Type 2 diabetes.
© 2023. The Author(s).
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
