

Neratinib + fulvestrant + trastuzumab for HR-positive, HER2-negative, HER2-mutant metastatic breast cancer: outcomes and biomarker analysis from the SUMMIT trial
- PMID: 37597578
- PMCID: PMC11335023
- DOI: 10.1016/j.annonc.2023.08.003
Neratinib + fulvestrant + trastuzumab for HR-positive, HER2-negative, HER2-mutant metastatic breast cancer: outcomes and biomarker analysis from the SUMMIT trial
Abstract
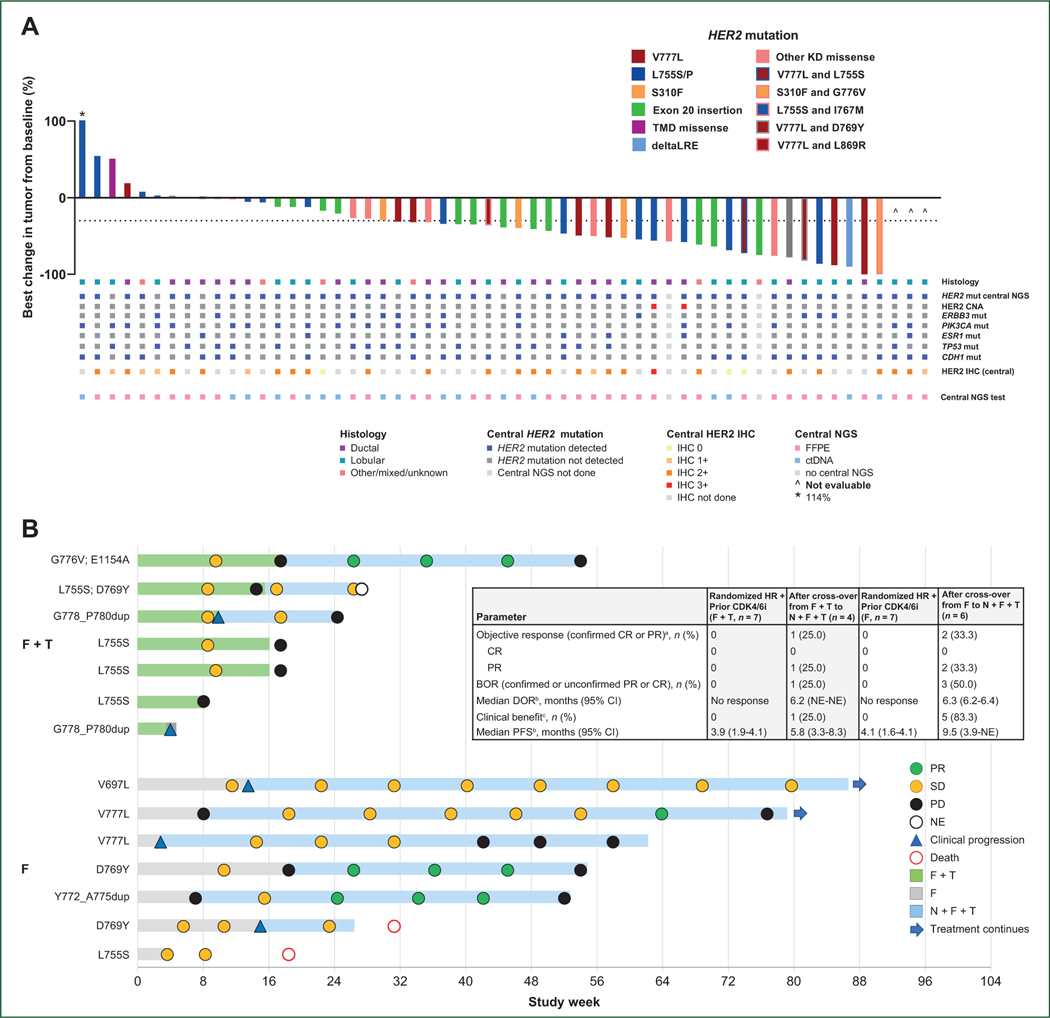
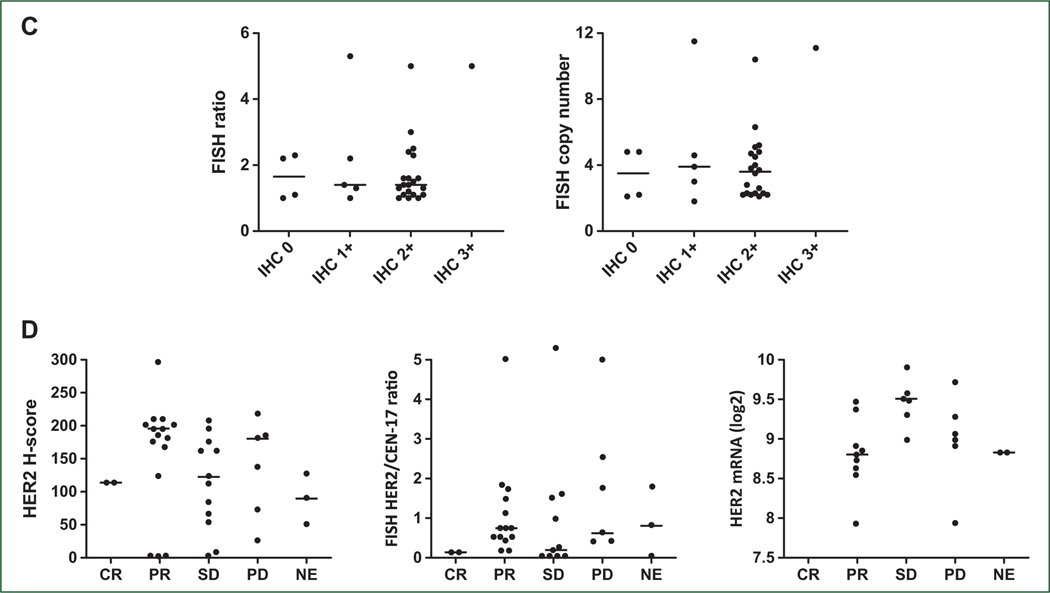
Background: HER2 mutations are targetable alterations in patients with hormone receptor-positive (HR+) metastatic breast cancer (MBC). In the SUMMIT basket study, patients with HER2-mutant MBC received neratinib monotherapy, neratinib + fulvestrant, or neratinib + fulvestrant + trastuzumab (N + F + T). We report results from 71 patients with HR+, HER2-mutant MBC, including 21 (seven in each arm) from a randomized substudy of fulvestrant versus fulvestrant + trastuzumab (F + T) versus N + F + T.
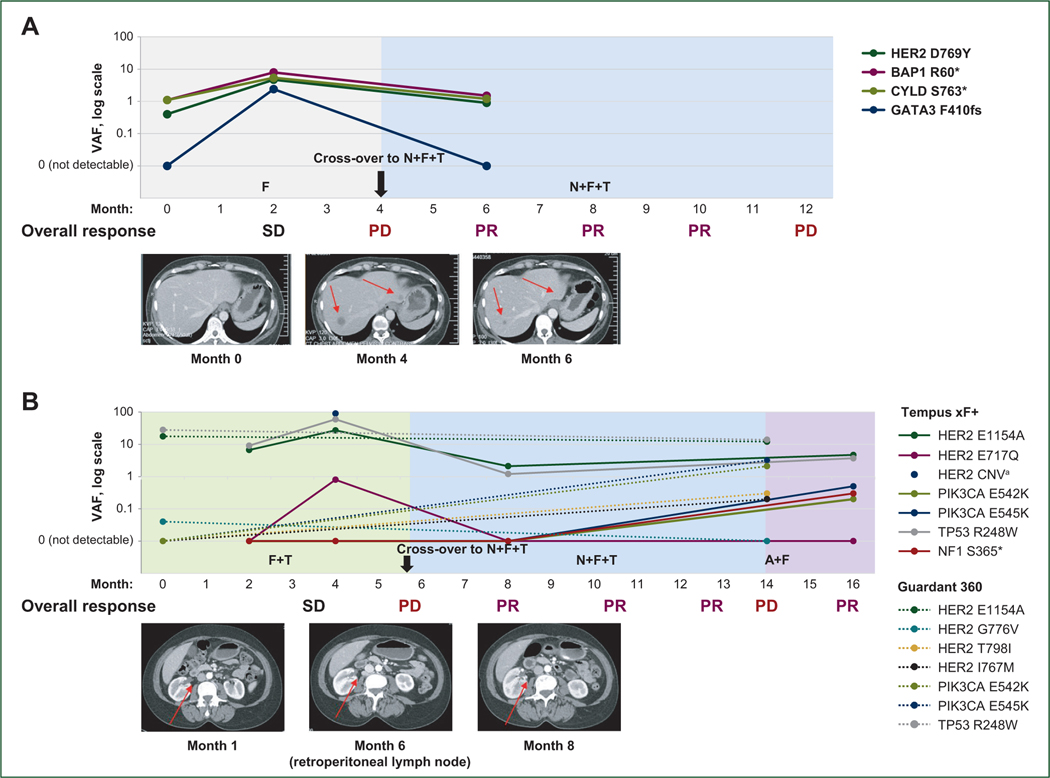
Patients and methods: Patients with HR+ HER2-negative MBC with activating HER2 mutation(s) and prior cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) therapy received N + F + T (oral neratinib 240 mg/day with loperamide prophylaxis, intramuscular fulvestrant 500 mg on days 1, 15, and 29 of cycle 1 then q4w, intravenous trastuzumab 8 mg/kg then 6 mg/kg q3w) or F + T or fulvestrant alone. Those whose disease progressed on F + T or fulvestrant could cross-over to N + F + T. Efficacy endpoints included investigator-assessed objective response rate (ORR), clinical benefit rate (RECIST v1.1), duration of response, and progression-free survival (PFS). Plasma and/or formalin-fixed paraffin-embedded tissue samples were collected at baseline; plasma was collected during and at end of treatment. Extracted DNA was analyzed by next-generation sequencing.
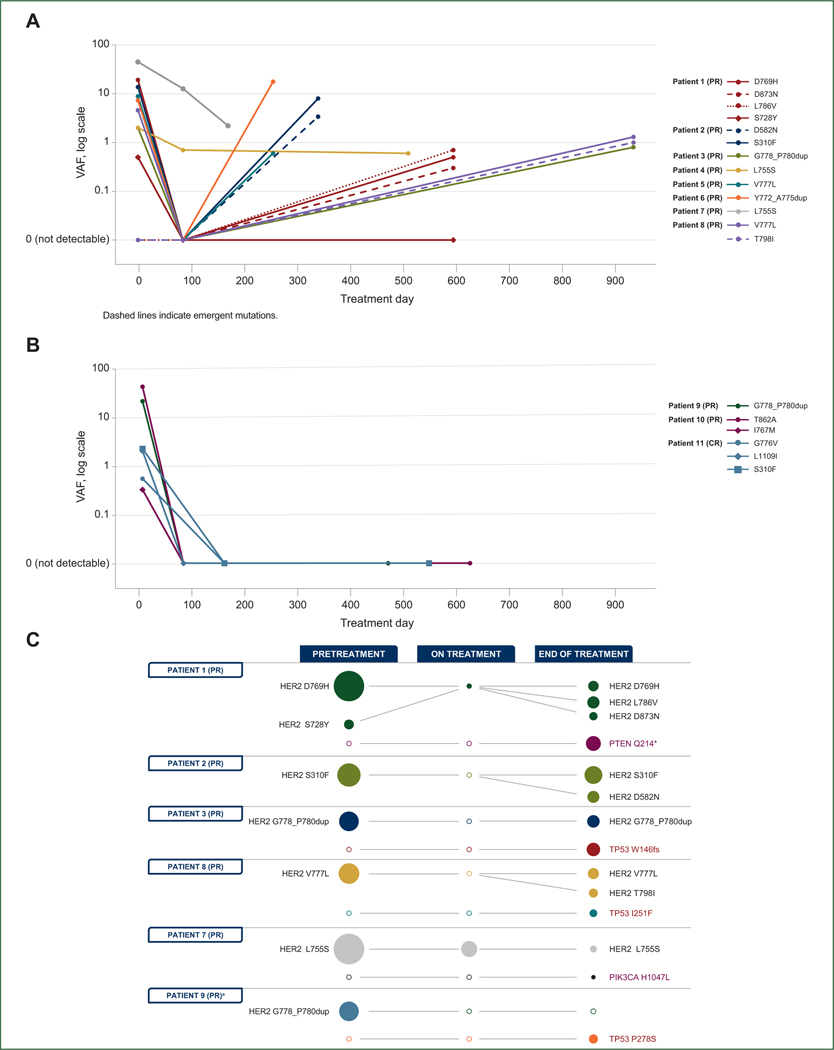
Results: ORR for 57 N + F + T-treated patients was 39% [95% confidence interval (CI) 26% to 52%); median PFS was 8.3 months (95% CI 6.0-15.1 months). No responses occurred in fulvestrant- or F + T-treated patients; responses in patients crossing over to N + F + T supported the requirement for neratinib in the triplet. Responses were observed in patients with ductal and lobular histology, 1 or ≥1 HER2 mutations, and co-occurring HER3 mutations. Longitudinal circulating tumor DNA sequencing revealed acquisition of additional HER2 alterations, and mutations in genes including PIK3CA, enabling further precision targeting and possible re-response.
Conclusions: The benefit of N + F + T for HR+ HER2-mutant MBC after progression on CDK4/6is is clinically meaningful and, based on this study, N + F + T has been included in the National Comprehensive Cancer Network treatment guidelines. SUMMIT has improved our understanding of the translational implications of targeting HER2 mutations with neratinib-based therapy.
Trial registration: ClinicalTrials.gov NCT01953926 NCT01670877 NCT03734029 NCT04639219 NCT05372614.
Keywords: ERBB2; HER2-mutant; hormone receptor-positive; metastatic breast cancer; neratinib.
Copyright © 2023 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure KJ: Consultant/Advisory Board: Novartis, AstraZeneca, Pfizer, BMS, Jounce Therapeutics, Taiho Oncology, Genentech/Roche, Lilly Pharmaceuticals/Loxo Oncology, AbbVie, Eisai, Blueprint Medicines, Seattle Genetics, Daiichi Sankyo, Gilead, Olema Pharmaceuticals, Sun Pharma Advanced Research Company Ltd., Menarini/Stemline, and Scorpion Therapeutics. Research Funding: Novartis, Genentech/Roche, AstraZeneca, Debio Pharmaceuticals, Pfizer, Lilly Pharmaceuticals/Loxo Oncology, Zymeworks, Gilead, Puma Biotechnology, Merck Pharmaceuticals, and Scorpion Therapeutics. HW: His institution received financial compensation on his behalf for advisory boards, lecture fees and/or consultancy fees from Daiichi Sankyo, Gilead, Lilly, Augustine Therapeutics, AstraZeneca, Immutep Pty, MSD, and Roche. He received travel support from Gilead, Daiichi Sankyo, and Pfizer. SAH: Contracted research paid to institution +/- editorial support for authorship: Ambrx, Arvinas, AstraZeneca, Bayer, Celcuity, Cytomx, Daiichi Sankyo, Dantari, Dignitana, Genentech/Roche, G1-Therapeutics, Gilead, Greenwich Life Sciences Inc., GSK, Immunomedics, Eli Lilly, Loxo, Macrogenics, Novartis, OBI Pharma, Orinove, Orum, Pfizer, Phoenix Molecular Designs, Ltd., Pieris, PUMA, Radius, Sanofi, Seattle Genetics/Seagen, and Zymeworks. Speaking: Daiichi Sankyo (2021). AG-Z: Advisory/Consultancy: AstraZeneca, Novartis, MSD, Pierre-Fabre, and Exact Science. Speaker Bureau/Expert testimony: Roche, AstraZeneca, Novartis, MSD, Pfizer, Lilly, and Pierre-Fabre. Research grant/Funding (institution): Pfizer. Travel/Accommodation/Expenses: Roche, Novartis, and Pfizer. NU: Consultant/Advisory Board: Novartis, Eli Lilly, BioTheranostics, Gilead. AB: Consultant: AstraZeneca, Pfizer, Novartis, Lilly, Genentech/Roche, Seagen, Daiichi Sankyo, Merck, Agendia, Sanofi, Puma, Myriad, and Gilead; research support: Agendia and AstraZeneca. HP: Research grants to institution: Adlai Nortye USA, Ambrx, Aprea Therapeutics AB, Array BioPharma, AstraZeneca, BJ Bioscience, Bristol-Myers Squibb, Daiichi Pharmaceutical, Elicio Therapeutics, Exelixis, Fate Therapeutics, Genentech, GlaxoSmithKline, Gossamer Bio, Hutchison MediPharma, ImmuneOncia Therapeutics, ImmunoGen, Mabspace Biosciences, MacroGenics, Merck, Mirati Therapeutics, Novartis Pharmaceuticals, Oncologie, PsiOxus Therapeutics, RePare Therapeutics, Seattle Genetics, Synermore Biologics, TopAlliance Biosciences, Turning Point Therapeutics, Vedanta Biosciences, Xencor. ESY: Research funding: Puma Biotechnology; Advisory boards: Bayer, Clovis; Consultant: AstraZeneca. IS: Institutional Research Funding: Roche/Genentech, Puma Biotechnology, MSD, Merck, AstraZeneca, Incyte, Orion, Genmab, Bristol-Myers Squibb, Bayer/Loxo Oncology, Lilly Pharmaceuticals/Loxo Oncology, Novartis, Pfizer, Amgen, Repare Therapeutics. Honoraria: AstraZeneca. Support for travel and meeting attendance: Roche, Novartis, Merck/Pfizer, Incyte, and AstraZeneca. SR: Consultant/Advisory board: Novartis, AstraZeneca, Gilead, and Daiichi Sankyo. MBh: Consulting/Advisory Board: Daiichi Sankyo, Merck, Pfizer, and AstraZeneca. SV: Funding from Pfizer directly to institution for conducting clinical trial. MA: Consulting or advisory role: Pfizer, AstraZeneca, Menarini, Novartis, Daiichi Sankyo, and Gilead. Speaker’s bureau: Pfizer, Novartis, and Gilead. Research funding: AstraZeneca. F-CB: Consulting or advisory role: Pfizer; AstraZeneca; Lilly; Novartis; Menarini; Sanofi; GSK; Rain Oncology; Caris Life Sciences; GE Healthcare; Exact Sciences; Gilead. Speaker's bureau: Pfizer; Novartis; AstraZeneca; Roche; Lilly; Rain Oncology; Daiichi Sankyo; and Menarini-Stemline. Research Funding: Novartis; Pfizer; Menarini Silicon Biosystems; Prolynx; Merck KGaA; and GE Healthcare. SL: Receives research funding to her institution from Novartis, Bristol Myers Squibb, Merck, Puma Biotechnology, Eli Lilly, Nektar Therapeutics, AstraZeneca, and Seattle Genetics. She has acted as consultant (not compensated) to Seattle Genetics, Novartis, Bristol Myers Squibb, Merck, AstraZeneca, Eli Lilly, Pfizer, Gilead Therapeutics, and Roche-Genentech. She has acted as consultant (paid to her institution) to Aduro Biotech, Novartis, GlaxoSmithKline, Roche-Genentech, AstraZeneca, Silverback Therapeutics, G1 Therapeutics, Puma Biotechnology, Inc., Pfizer, Gilead Therapeutics, Seattle Genetics, Daiichi Sankyo, Merck, Amunix, Tallac Therapeutics, Eli Lilly, and Bristol Myers Squibb. JC: Has taken part in advisory boards for Puma Biotechnology. His unit is the recipient of a peer-reviewed grant from Science Foundation Ireland (an Irish government organization) which is part-funded by Puma Biotechnology Inc. Neither he nor his spouse own Puma Biotechnology stock. MEB: Medical advisory board of Strata Oncology; Research funding from AbbVie, Arcus, Apollomics, Elevation Oncology, Endeavor, Genetech, Puma, Loxo Oncology, and Seagen. SAP-P: Clinical trial research support/grant funding through the institution from AbbVie, Inc., ABM Therapeutics, Inc., Acepodia, Inc., Alkermes, Aminex Therapeutics, Amphivena Therapeutics, Inc., BioMarin Pharmaceutical, Inc., Boehringer Ingelheim, Bristol-Myers Squibb, Cerulean Pharma, Inc., Chugai Pharmaceutical Co., Ltd., Curis, Inc., Cyclacel Pharmaceuticals, Daiichi Sankyo, Eli Lilly, ENB Therapeutics, Epigenetix Inc., Five Prime Therapeutics, F-Star Beta Limited, F-Star Therapeutics, Gene Quantum, Genmab A/S, Gilead Sciences, Inc., GlaxoSmithKline, Helix BioPharma Corp., Hengrui Pharmaceuticals, Co., Ltd., HiberCell, Inc., Immorna Biotherapeutics, Inc., Immunomedics, Inc., Incyte Corp., Jacobio Pharmaceuticals Co., Ltd., Jiangsu Simcere Pharmaceutical Co., Ltd., Lytix Biopharma AS, Medimmune, LLC., Medivation, Inc., Merck Sharp and Dohme Corp., Nectin Therapeutics, Ltd., Novartis Pharmaceuticals, Pieris Pharmaceuticals, Inc., Pfizer, Phanes Therapeutics, Principia Biopharma, Inc., Puma Biotechnology, Inc., Purinomia Biotech, Inc., Rapt Therapeutics, Inc., Replimune, Seattle Genetics, Silverback Therapeutics, Synlogic Therapeutics, Taiho Oncology, Tesaro, Inc., TransThera Bio, ZielBio, Inc., NCI/NIH, P30CA016672—Core Grant (CCSG Shared Resources); and consulting fees from CRC Oncology. JMS: Research grant support: AstraZeneca and Strata Oncology. SC: Advisory/Consultancy: Novartis, F. Hoffmann-La Roche, Pfizer, Eli Lilly, AstraZeneca, Amgen, Gilead, Merck, and Exact Sciences. Research funding to the institution: Novartis, F. Hoffmann-La Roche, Pfizer, Genomic Health/Exact Sciences, AstraZeneca, Genentech, Celgene, Amgen, BMS, Merck, Sanofi, Puma, and Gilead. CS: Consulting, advisory role or travel grants from: AstraZeneca, AX'Consulting, Byondis B.V, Daiichi Sankyo, Eisai, Exact Sciences, Exeter Pharma, F. Hoffmann-La Roche Ltd., Lilly, MediTech, Merck Sharp & Dohme, Novartis, Pfizer, Philips, Pierre-Fabre, PintPharma, Puma Biotechnology, Seagen, and Zymeworks. JAG-S: Consulting or advisory role: Novartis Pharmaceuticals Corporation, AstraZeneca, Lilly, Seagen, Daiichi Sankyo, Gilead Sciences, Exact Sciences, and Stemline Menarini; speakers bureau: Novartis Pharmaceuticals Corporation, Lilly, AstraZeneca, and Stemline Menarini; travel, accommodations, expenses: Daiichi Sankyo, Gilead Sciences, and Exact Sciences. VG: Advisory Board: Boehringer. Research Funding: Bayer, Boehringer, Roche. Institutional Funding: Genentech, Merck Serono, Roche, Beigene, Bayer, Servier, Lilly, Novartis, Takeda, Astellas, Fibrogen, Amcure, Natera, Sierra Oncology, AstraZeneca, Medimmune, BMS, and MSD. ENG-Y: Honoraria from Novartis, Pfizer, Eli Lilly, MSD, and AstraZeneca. CM: Has received research grants from Puma Biotechnology and Pfizer. She received consulting fees from AstraZeneca, Olaris, Novartis, and Sanofi. ABH: Reports stock and other ownership interests in Pfizer (immediate family member) and research funding from Takeda. JWG: has received institutional research funding from Puma Biotechnology Inc. RB: Receives research grant from Puma; has performed consulting for Genentech. JSKB: Employee (and stockholder) of Tempus Labs. LDE, DD, AF, and AW: Employees and stockholders of Puma Biotechnology. CLA: Has received research grants from Pfizer, Lilly, and Takeda. He serves or has served as scientific advisor to Novartis, Lilly, AstraZeneca, Daiichi Sankyo, Merck, Immunomedics, OrigiMed, Sanofi, TAIHO Oncology, and Puma Biotechnology. DBS: Has served as a consultant for/received honorarium from Pfizer, Vividion Therapeutics, Scorpion Therapeutics, FORE Therapeutics, Fog Pharma, Elsie Biotechnologies, Fog Pharma, Rain Oncology, Function Oncology, and BridgeBio. All other authors have declared no conflicts of interest. Data Sharing The authors declare that the data supporting the findings of this study are available within the article. Qualified researchers and study participants may submit requests for other study documentation and clinical trial data to clinicaltrials@pumabiotechnology.com for consideration.
Figures
References
-
- Kurozumi S, Alsaleem M, Monteiro CJ, et al. Targetable ERBB2 mutation status is an independent marker of adverse prognosis in estrogen receptor positive, ERBB2 non-amplified primary lobular breast carcinoma: a retrospective in silico analysis of public datasets. Breast Cancer Res. 2020;22:85. - PMC - PubMed
-
- Schram A, Won HH, Andre F, et al. Abstract LB-103: landscape of somatic ERBB2 mutations: findings from AACR GENIE and comparison to ongoing ERBB2 mutant basket study. Cancer Res. 2017;77(suppl 13): LB103.
-
- Desmedt C, Zoppoli G, Gundem G, et al. Genomic characterization of primary invasive lobular breast cancer. J Clin Oncol. 2016;34(16):1872–1881. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
