

Altered insulin secretion dynamics relate to oxidative stress and inflammasome activation in children with obesity and insulin resistance
- PMID: 37599368
- PMCID: PMC10440893
- DOI: 10.1186/s12967-023-04337-7
Altered insulin secretion dynamics relate to oxidative stress and inflammasome activation in children with obesity and insulin resistance
Abstract
Background: Insulin resistance (IR) is considered the main driver of obesity related metabolic complications, and is related to oxidative stress and inflammation, which in turn promote each other. There is currently no specific definition of IR in children, rather, that for adult population is used by pediatric endocrinologists instead. Altered insulin secretion dynamics are associated with worse metabolic profiles and type 2 diabetes mellitus development, thus we aimed to test whether insulin response relates to oxidative stress and inflammation in children.
Methods: We conducted a case-control study, including 132 children classified as follows: 33 children without obesity (Lean); 42 with obesity but no IR according to the American Diabetes Association criteria for adults (OBIR-); 25 with obesity and IR and an early insulin response to an oral glucose tolerance test (OGTT) (EP-OBIR +); 32 with obesity, IR, and a late insulin peak (LP-OBIR +); and studied variables associated with lipid and carbohydrate metabolism, oxidative stress, inflammation and inflammasome activation.
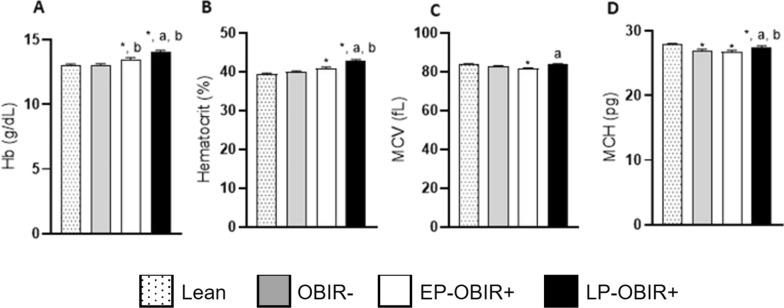
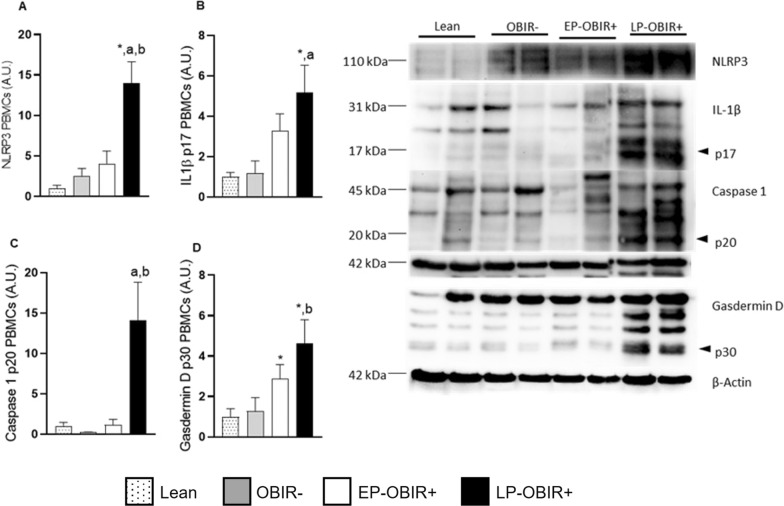
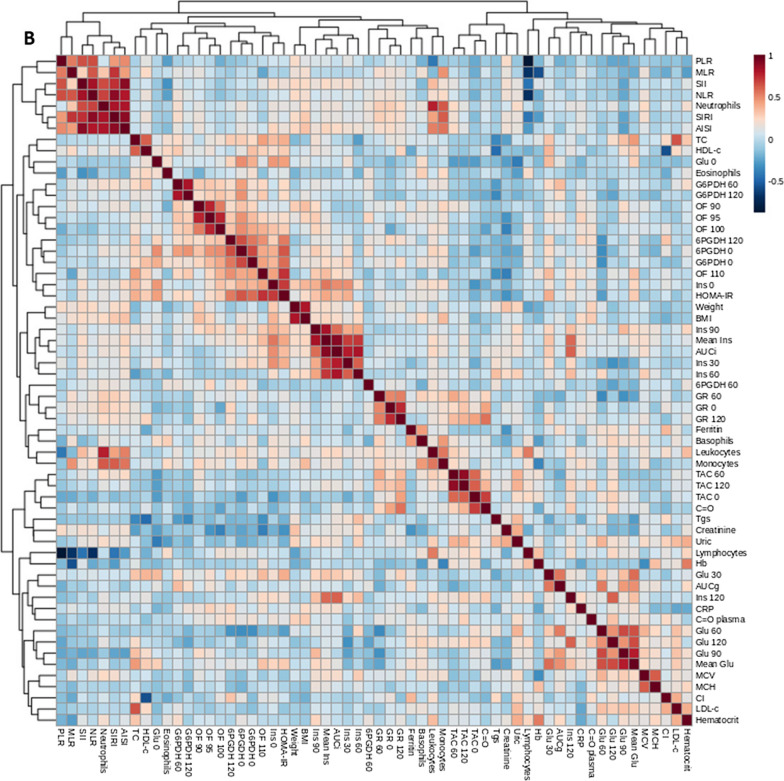
Results: The measured parameters of children with obesity, IR, and an early insulin response were similar to those of children with obesity but without IR. It was late responders who presented an impaired antioxidant system and elevated oxidative damage in erythrocytes and plasma, and inflammasome activation at their white blood cells, despite lower classical inflammation markers. Increased uric acid levels seems to be one of the underlying mechanisms for inflammasome activation.
Conclusions: It is insulin response to an OGTT that identifies children with obesity suffering oxidative stress and inflammasome activation more specifically. Uric acid could be mediating this pathological inflammatory response by activating NLRP3 in peripheral blood mononuclear cells.
Keywords: Childhood obesity; Inflammasome activation; Insulin resistance; Oral glucose tolerance test; Oxidative stress.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests related with this work.
Figures






References
-
- Soriano JB, Rojas-Rueda D, Alonso J, Antó JM, Cardona PJ, Fernández E, et al. La carga de enfermedad en España: resultados del estudio de la carga global de las enfermedades 2016. Med Clin (Barc) 2018;151(5):171–190. - PubMed
-
- Martos-Moreno GÁ, Gil-Campos M, Bueno G, Bahillo P, Bernal S, Feliu A, et al. Obesity associated metabolic impairment is evident at early ages: Spanish collaborative study. Nutr Hosp. 2014;30(4):787–793. - PubMed
-
- Gerich JE. Is reduced first-phase insulin release the earliest detectable abnormality in individuals destined to develop type 2 diabetes? Diabetes. 2002;51(suppl_1):S117–21. - PubMed
-
- Sun Y, Han J, Lin Z, Song L, Wang C, Jia W. Delayed insulin secretion response during an OGTT is associated with an increased risk for incidence of diabetes in NGT subjects. J Diabetes Complicat. 2016;30(8):1537–43. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
