

The effects of acarbose treatment on cardiovascular risk factors in impaired glucose tolerance and diabetic patients: a systematic review and dose-response meta-analysis of randomized clinical trials
- PMID: 37599681
- PMCID: PMC10433190
- DOI: 10.3389/fnut.2023.1084084
The effects of acarbose treatment on cardiovascular risk factors in impaired glucose tolerance and diabetic patients: a systematic review and dose-response meta-analysis of randomized clinical trials
Abstract
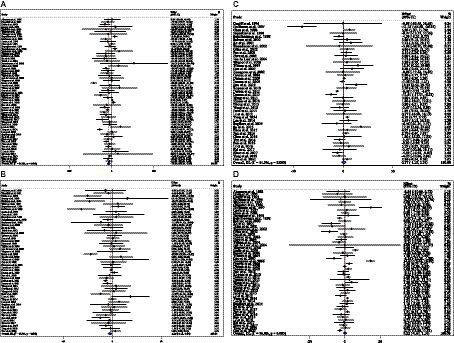
Acarbose (ACB) seems to be an effective drug in the management of cardiovascular risk factors. However, no previous meta-analysis of randomized controlled trials (RCTs) has been done to evaluate the effects of ACB on cardiovascular risk factors on impaired glucose tolerance (IGT), type 2 diabetes mellitus (T2D), and type 1 diabetes mellitus (T1D). We comprehensively searched electronic databases including Scopus, Web of Science, and PubMed for RCTs for related keywords up to September 2022. A random-effects model was used to estimate the weighted mean difference (WMD) and 95% confidence interval (CI). The pooled analysis demonstrated that ACB treatment had a significant effect on fasting blood glucose (FBG) (WMD = -3.55 mg/dL; 95%CI: -6.29, -0.81; p = 0.011), fasting insulin (WMD = -6.73 pmoL/L; 95%CI: -10.37, -3.10; p < 0.001), HbA1c [WMD = -0.32%; 95%CI: -0.45, -0.20; p < 0.001], body weight (WMD = -1.25 kg; 95%CI: -1.79, -0.75; p < 0.001), body mass index (BMI) (WMD = -0.64 kg/m2; 95%CI: -0.92, -0.37; p < 0.001), tumor necrosis factor-alpha (TNF-α) (WMD = -2.70 pg/mL, 95%CI: -5.25, -0.16; p = 0.037), leptin (WMD = -1.58 ng/mL; 95%CI: -2.82, -0.35; p = 0.012), alanine transaminase (ALT) (WMD = 0.71 U/L; 95%CI: -0.31, 1.85; p = 0.164), triglyceride (TG) (WMD = -13.89 mg/dL; 95%CI: -20.69, -7.09; p < 0.001), total cholesterol (TC) (WMD = -2.26 mg/dL; 95%CI: -4.18, -0.34; p = 0.021), systolic blood pressure (SBP) (WMD = -1.29 mmHg; 95%CI: -2.44, -0.15; p = 0.027), and diastolic blood pressure (DBP) (WMD = 0.02 mmHg; 95%CI: -0.41, 0.45; p = 0.925) in an intervention group, compared with a placebo group. The non-linear dose-response analysis showed that ACB reduces the TC in trial duration by >50 weeks, and 180 mg/day is more effective for the decrement of CRP. ACB can improve lipid profiles, glycemic indices, anthropometric indices, and inflammatory markers in T2D, T1D, and IGT patients.
Keywords: acarbose; cardiovascular risk factors; diabetic patients; meta-analysis; systematic review.
Copyright © 2023 Zamani, Nikbaf-Shandiz, Aali, Rasaei, Zarei, Shiraseb and Asbaghi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






References
-
- Giedrimiene D, King R. Abstract 207: burden of cardiovascular disease (CVD) on economic cost. Comparison of outcomes in US and Europe. Circ Cardiovasc Qual Outcomes. (2017) 10:A207. doi: 10.1161/circoutcomes.10.suppl_3.207 - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous