

Large-scale identification of undiagnosed hepatic steatosis using natural language processing
- PMID: 37599905
- PMCID: PMC10432816
- DOI: 10.1016/j.eclinm.2023.102149
Large-scale identification of undiagnosed hepatic steatosis using natural language processing
Abstract
Background: Nonalcoholic fatty liver disease (NAFLD) is a major cause of liver-related morbidity in people with and without diabetes, but it is underdiagnosed, posing challenges for research and clinical management. Here, we determine if natural language processing (NLP) of data in the electronic health record (EHR) could identify undiagnosed patients with hepatic steatosis based on pathology and radiology reports.
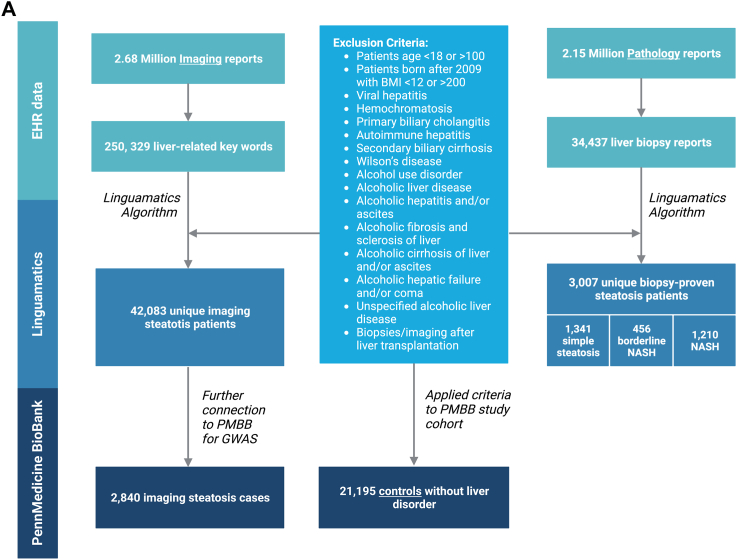
Methods: A rule-based NLP algorithm was built using a Linguamatics literature text mining tool to search 2.15 million pathology report and 2.7 million imaging reports in the Penn Medicine EHR from November 2014, through December 2020, for evidence of hepatic steatosis. For quality control, two independent physicians manually reviewed randomly chosen biopsy and imaging reports (n = 353, PPV 99.7%).
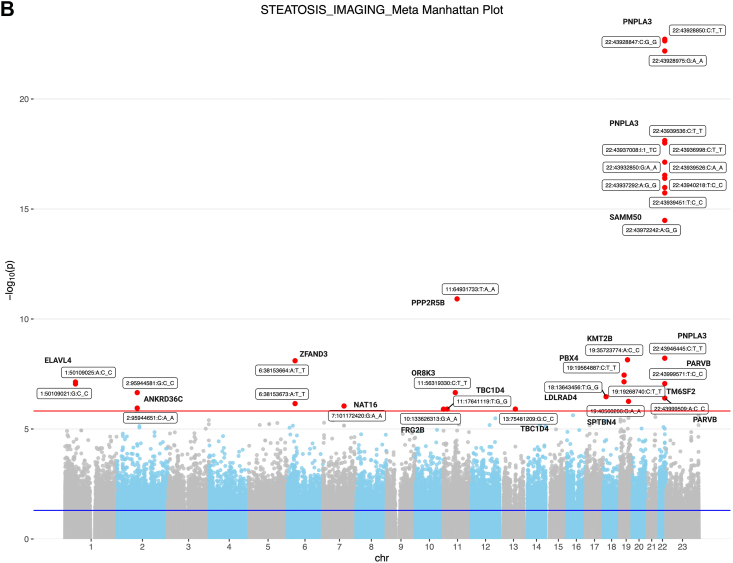
Findings: After exclusion of individuals with other causes of hepatic steatosis, 3007 patients with biopsy-proven NAFLD and 42,083 patients with imaging-proven NAFLD were identified. Interestingly, elevated ALT was not a sensitive predictor of the presence of steatosis, and only half of the biopsied patients with steatosis ever received an ICD diagnosis code for the presence of NAFLD/NASH. There was a robust association for PNPLA3 and TM6SF2 risk alleles and steatosis identified by NLP. We identified 234 disorders that were significantly over- or underrepresented in all subjects with steatosis and identified changes in serum markers (e.g., GGT) associated with presence of steatosis.
Interpretation: This study demonstrates clear feasibility of NLP-based approaches to identify patients whose steatosis was indicated in imaging and pathology reports within a large healthcare system and uncovers undercoding of NAFLD in the general population. Identification of patients at risk could link them to improved care and outcomes.
Funding: The study was funded by US and German funding sources that did provide financial support only and had no influence or control over the research process.
Keywords: Biopsy; EHR; Liver disease; NAFLD; Natural language processing.
© 2023 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Chalasani N., Younossi Z., Lavine J.E., et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American association for the study of liver diseases, American college of gastroenterology, and the American gastroenterological association. Hepatology. 2012;55(6):2005–2023. doi: 10.1002/hep.25762. - DOI - PubMed
-
- Vujkovic M., Ramdas S., Lorenz K.M., et al. A multiancestry genome-wide association study of unexplained chronic ALT elevation as a proxy for nonalcoholic fatty liver disease with histological and radiological validation. Nat Genet. 2022;54(6):761–771. doi: 10.1038/s41588-022-01078-z. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
