

Thrombotic and hemorrhagic complications of COVID-19 in adults hospitalized in high-income countries compared with those in adults hospitalized in low- and middle-income countries in an international registry
- PMID: 37601011
- PMCID: PMC10439444
- DOI: 10.1016/j.rpth.2023.102142
Thrombotic and hemorrhagic complications of COVID-19 in adults hospitalized in high-income countries compared with those in adults hospitalized in low- and middle-income countries in an international registry
Abstract
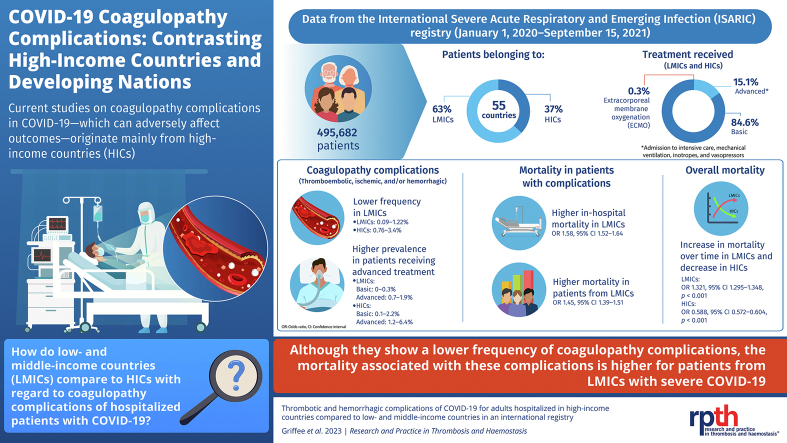
Background: COVID-19 has been associated with a broad range of thromboembolic, ischemic, and hemorrhagic complications (coagulopathy complications). Most studies have focused on patients with severe disease from high-income countries (HICs).
Objectives: The main aims were to compare the frequency of coagulopathy complications in developing countries (low- and middle-income countries [LMICs]) with those in HICs, delineate the frequency across a range of treatment levels, and determine associations with in-hospital mortality.
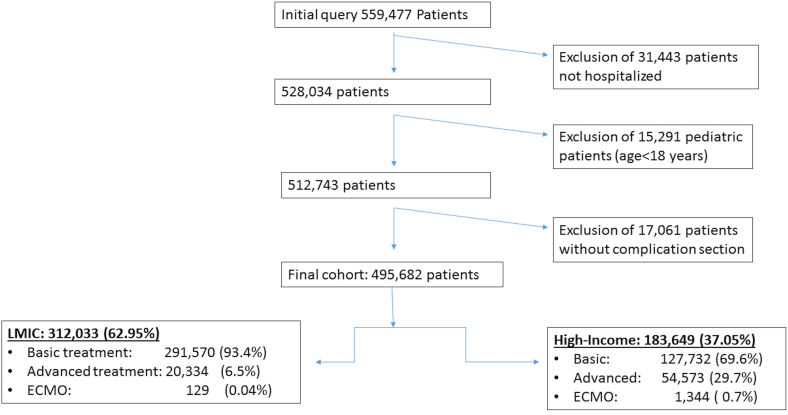
Methods: Adult patients enrolled in an observational, multinational registry, the International Severe Acute Respiratory and Emerging Infections COVID-19 study, between January 1, 2020, and September 15, 2021, met inclusion criteria, including admission to a hospital for laboratory-confirmed, acute COVID-19 and data on complications and survival. The advanced-treatment cohort received care, such as admission to the intensive care unit, mechanical ventilation, or inotropes or vasopressors; the basic-treatment cohort did not receive any of these interventions.
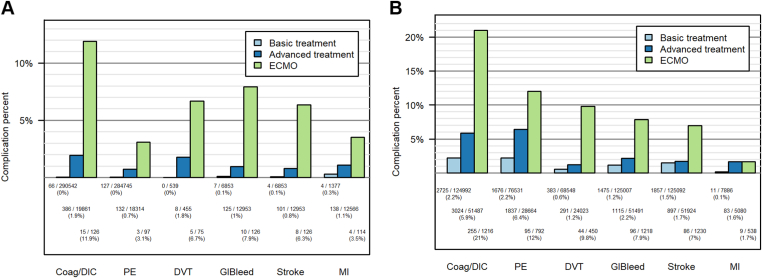
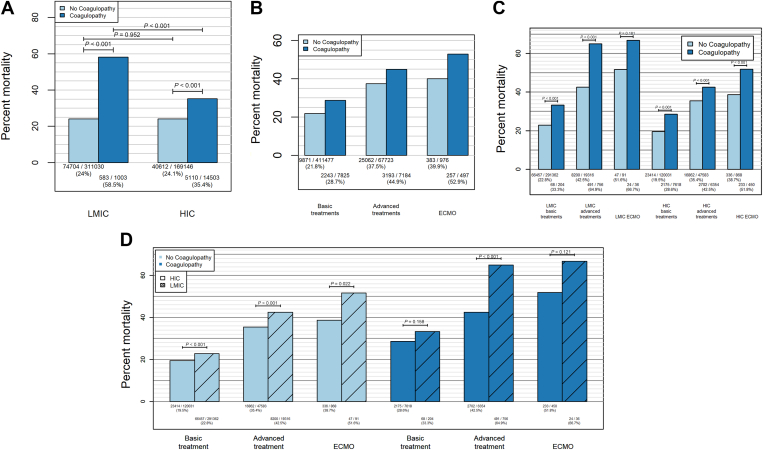
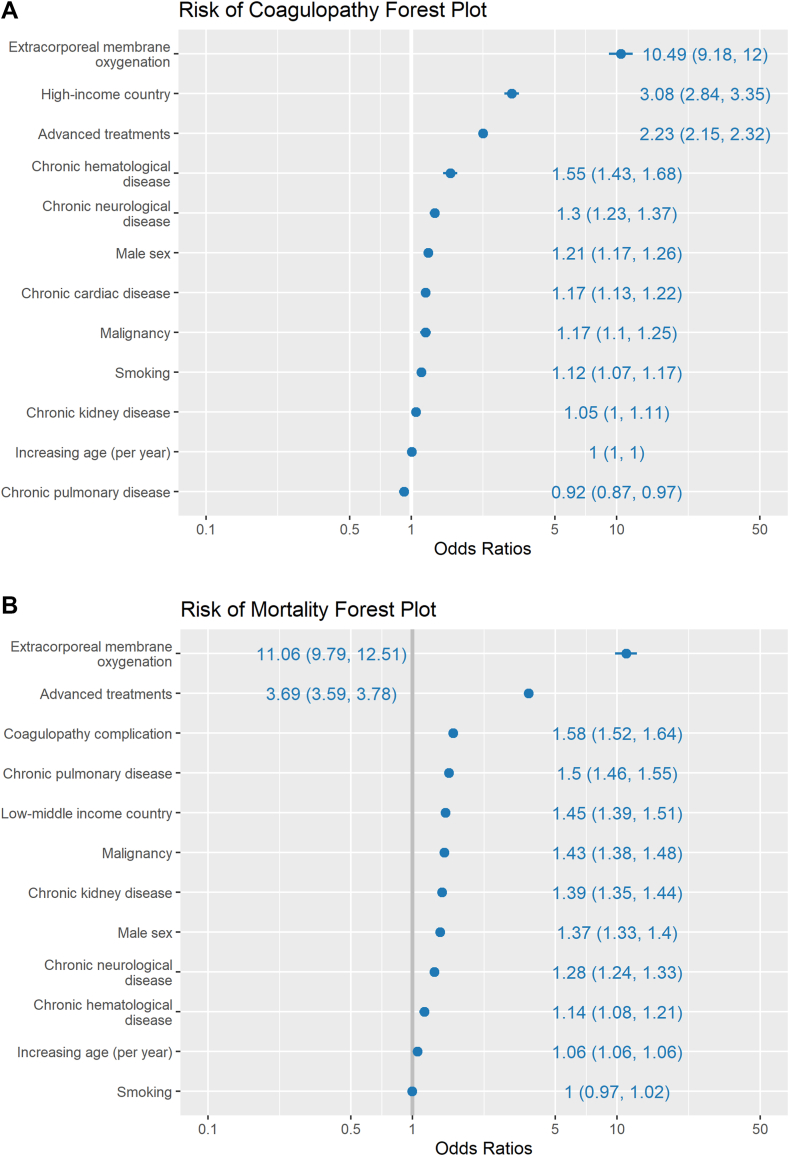
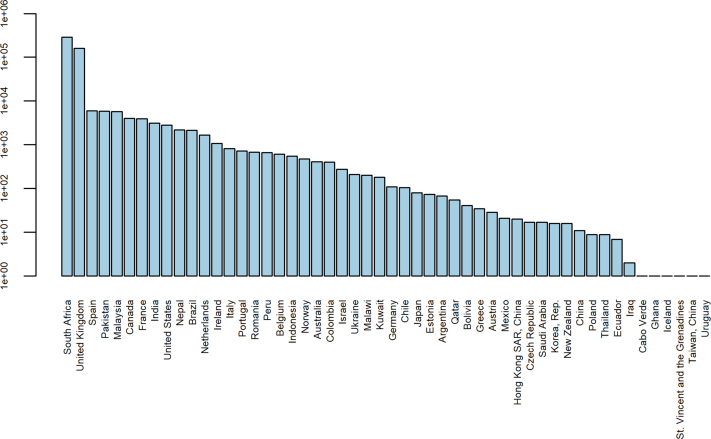
Results: The study population included 495,682 patients from 52 countries, with 63% from LMICs and 85% in the basic treatment cohort. The frequency of coagulopathy complications was higher in HICs (0.76%-3.4%) than in LMICs (0.09%-1.22%). Complications were more frequent in the advanced-treatment cohort than in the basic-treatment cohort. Coagulopathy complications were associated with increased in-hospital mortality (odds ratio, 1.58; 95% CI, 1.52-1.64). The increased mortality associated with these complications was higher in LMICs (58.5%) than in HICs (35.4%). After controlling for coagulopathy complications, treatment intensity, and multiple other factors, the mortality was higher among patients in LMICs than among patients in HICs (odds ratio, 1.45; 95% CI, 1.39-1.51).
Conclusion: In a large, international registry of patients hospitalized for COVID-19, coagulopathy complications were more frequent in HICs than in LMICs (developing countries). Increased mortality associated with coagulopathy complications was of a greater magnitude among patients in LMICs. Additional research is needed regarding timely diagnosis of and intervention for coagulation derangements associated with COVID-19, particularly for limited-resource settings.
Keywords: COVID-19; SARS-CoV-2; developing countries; disseminated intravascular coagulation; hemorrhage; ischemic stroke; thromboembolism; thrombosis.
© 2023 The Author(s).
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
