

Direct oral anticoagulants or vitamin K antagonists in emergencies: comparison of management in an observational study
- PMID: 37601024
- PMCID: PMC10439397
- DOI: 10.1016/j.rpth.2023.100196
Direct oral anticoagulants or vitamin K antagonists in emergencies: comparison of management in an observational study
Abstract
Background: Restoring hemostasis in patients on oral anticoagulants presenting with major hemorrhage (MH) or before surgical intervention has changed, with the replacement of vitamin K antagonist (VKA) with direct oral anticoagulants (DOACs).
Objectives: To observe the difference in urgent hemostatic management between patients on VKA and those on DOACs.
Methods: A multicenter observational study evaluated the variation in laboratory testing, hemostatic management, mortality, and hospital length of stay (LOS) in patients on VKA or DOACs presenting with MH or urgent hemostatic restoration.
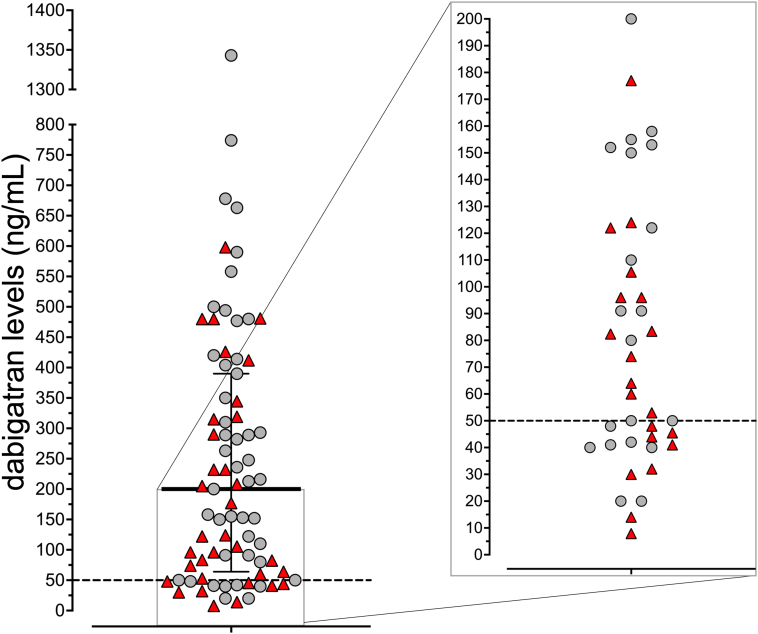
Results: Of the 1194 patients analyzed, 783 had MH (61% VKA) and 411 required urgent hemostatic restoration before surgery (56% VKA). Compared to the international normalized ratio (97.6%), plasma DOAC levels were measured less frequently (<45%), and the time taken from admission for the coagulation sample to reach the laboratory varied widely (median, 52.3 minutes; IQR, 24.8-206.7). No significant plasma DOAC level (<50 ng/mL) was found in up to 19% of patients. There was a poor relationship between plasma DOAC level and the usage of a hemostatic agent. When compared with patients receiving VKA (96.5%) or dabigatran (93.7%), fewer patients prescribed a factor Xa inhibitor (75.5%) received a prohemostatic reversal agent. The overall 30-day mortality for MH (mean: 17.8%) and length of stay (LOS) (median: 8.7 days) was similar between VKA and DOAC patients.
Conclusion: In DOAC patients, when compared to those receiving VKA, plasma DOAC levels were measured less frequently than the international normalized ratio and had a poor relationship with administering a hemostatic reversal agent. In addition, following MH, mortality and LOS were similar between VKA and DOAC patients.
Keywords: anticoagulants; coagulation; dabigatran; hemorrhage; hemostatics.
© 2023 The Authors.
Figures



References
-
- Ruff C.T., Giugliano R.P., Braunwald E., Hoffman E.B., Deenadayalu N., Ezekowitz M.D., et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383:955–962. - PubMed
-
- Lui B., Wee B., Lai J., Khattak Z., Kwok A., Donarelli C., et al. A ten-year review of the impact of the transition from warfarin to direct oral anticoagulant—has venous thromboembolism treatment become safer? Thromb Res. 2022;219:112–120. - PubMed
LinkOut - more resources
Full Text Sources
