

Explaining the poor-rich gap in anthropometric failure among children in India: An econometric analysis of the NFHS, 2021 and 2016
- PMID: 37601140
- PMCID: PMC10433217
- DOI: 10.1016/j.ssmph.2023.101482
Explaining the poor-rich gap in anthropometric failure among children in India: An econometric analysis of the NFHS, 2021 and 2016
Abstract
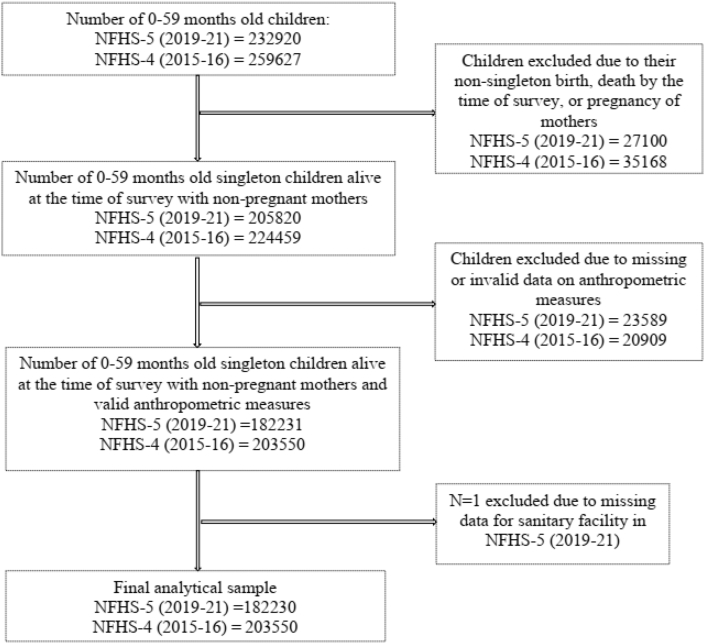
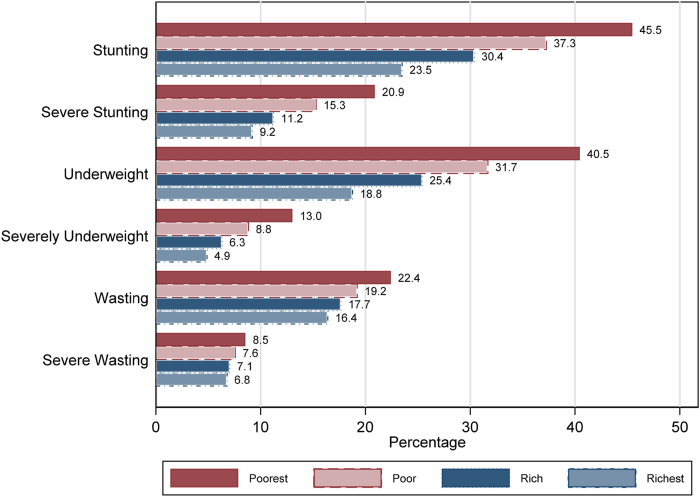
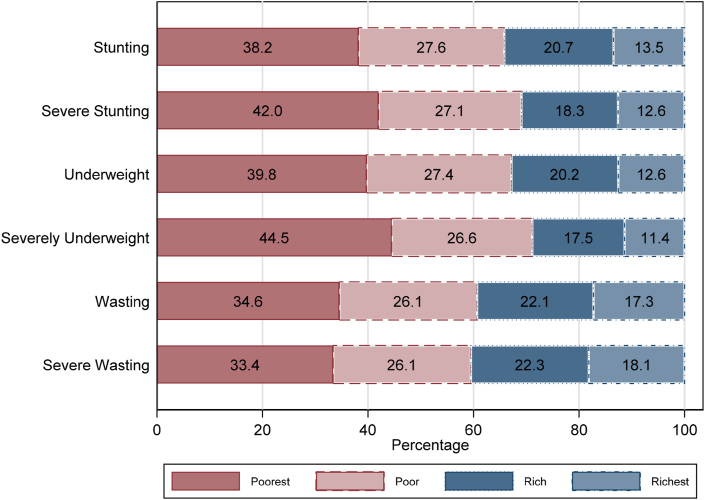
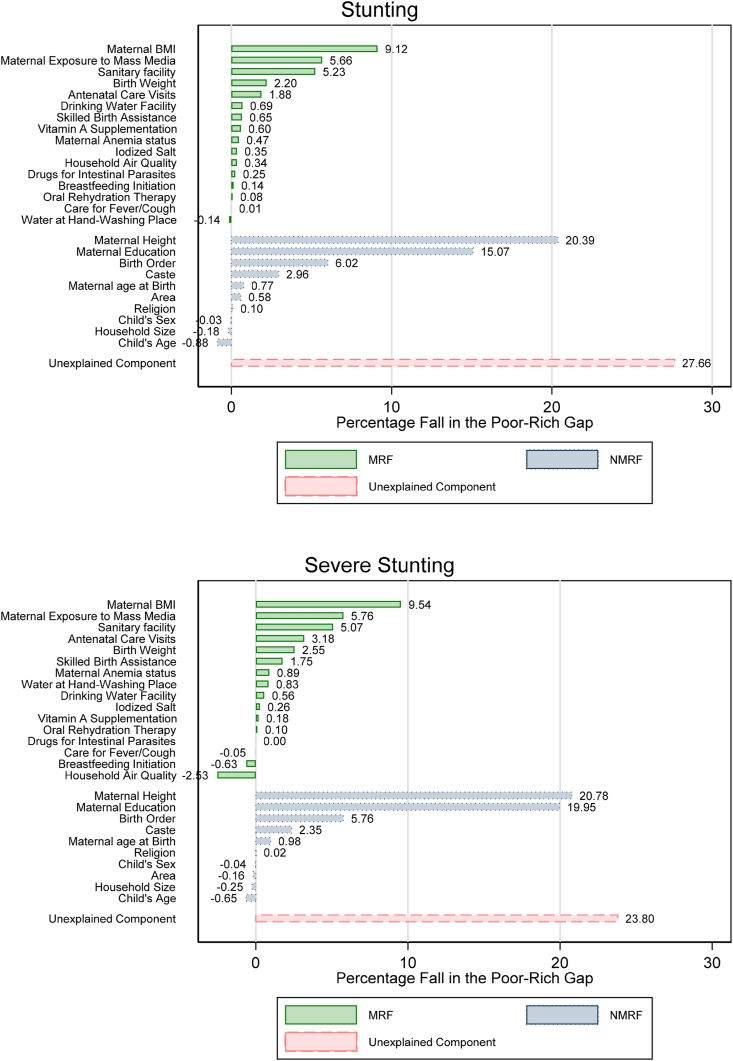
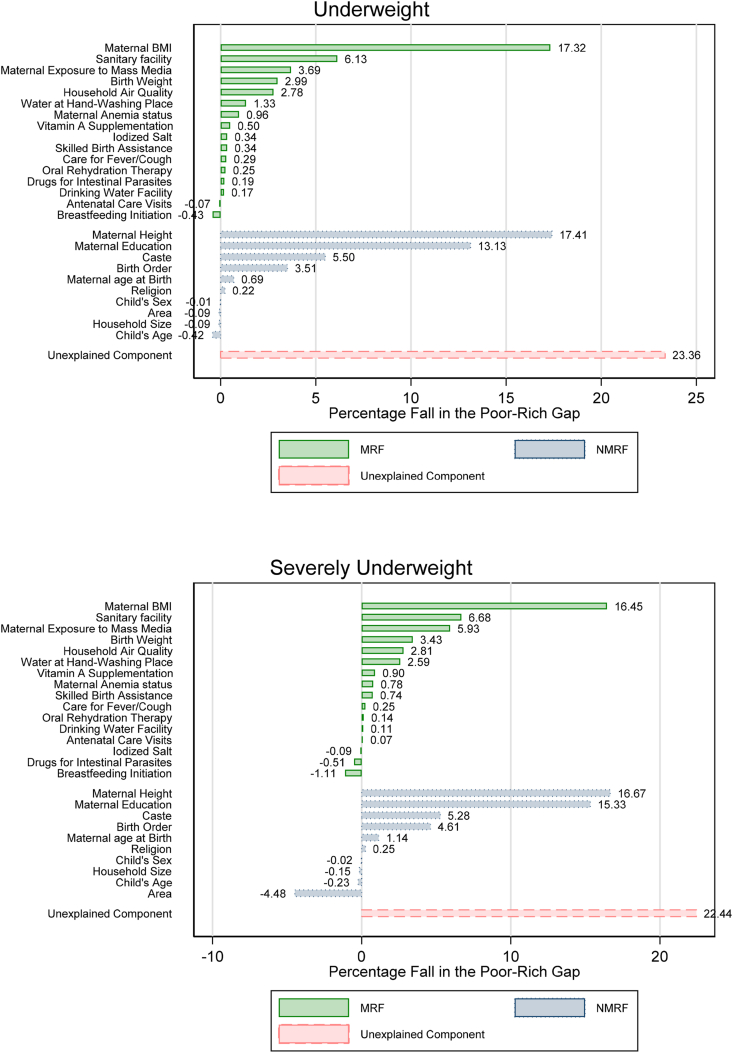
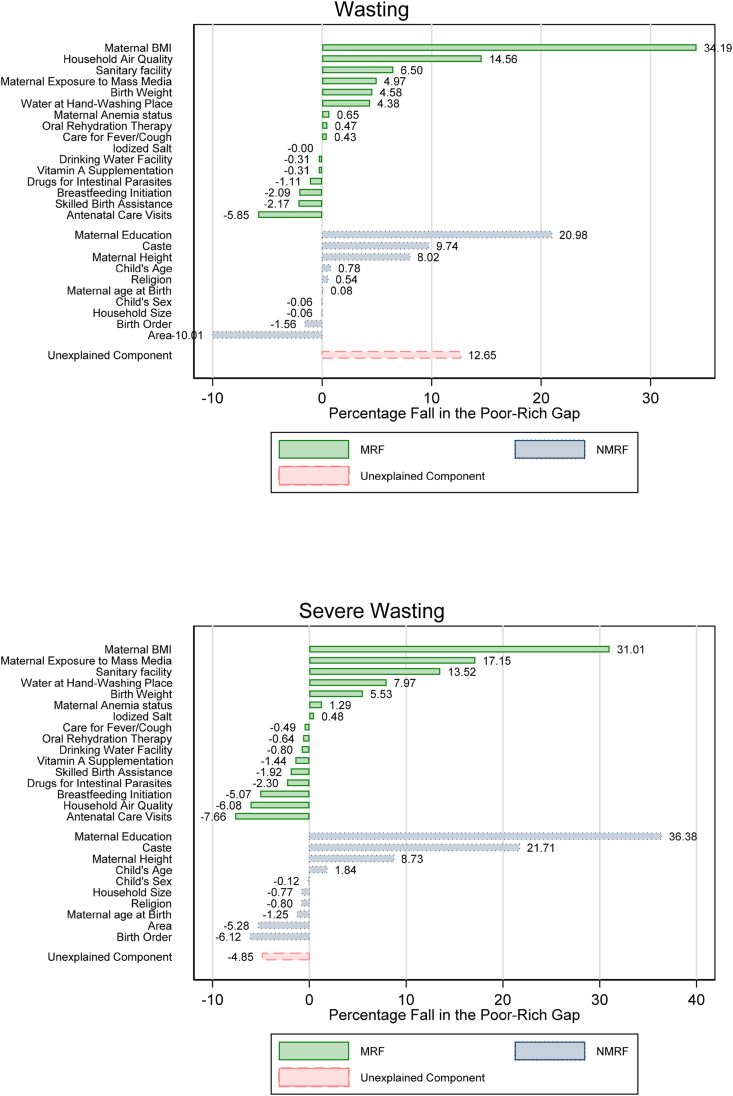
Wealth inequality in anthropometric failure is a persistent concern for policymakers in India. This necessitates a comprehensive analysis and identification of various risk factors that can explain the poor-rich gap in anthropometric failure among children in India. We analyze the fifth and fourth rounds of the Indian National Family Health Survey collected from June 2019 to April 2021 and January 2015 to December 2016, respectively. Two samples of children aged 0-59 and 6-23 months old with singleton birth, alive at the time of the survey with non-pregnant mothers, and with valid data on stunting, severe stunting, underweight, severely underweight, wasting, and severe wasting are included in the analytical samples from both rounds. We estimate the wealth gradients and distribution of wealth among children with anthropometric failure. Wealth gap in anthropometric failure is identified using logistic regression analysis. The contribution of risk factors in explaining the poor-rich gap in AF is estimated by the multivariate decomposition analysis. We observe a negative wealth gradient for each measure of anthropometric failure. Wealth distributions indicate that at least 60% of the population burden of anthropometric failure is among the poor and poorest wealth groups. Even among children with similar modifiable risk factors, children from poor and poorest backgrounds have a higher prevalence of anthropometric failure compared to children from the richest backgrounds. Maternal BMI, exposure to mass media, and access to sanitary facility are the most significant risk factors that explain the poor-rich gap in anthropometric failure. This evidence suggests that the burden of anthropometric failure and its risk factors are unevenly distributed in India. The policy interventions focusing on maternal and child health, implemented with a targeted approach prioritizing the vulnerable groups, can only partially bridge the poor-rich gap in anthropometric failure. The role of anti-poverty programs and growth is essential to narrow this gap in anthropometric failure.
Keywords: Anthropometric failure; India; Poor-rich gap; Risk factors; Wealth inequality.
© 2023 The Authors.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Inequality in child undernutrition among urban population in India: a decomposition analysis.BMC Public Health. 2020 Dec 3;20(1):1852. doi: 10.1186/s12889-020-09864-2. BMC Public Health. 2020. PMID: 33272222 Free PMC article.
-
Socio-economic inequality in anthropometric failure among children aged under 5 years in India: evidence from the Comprehensive National Nutrition Survey 2016-18.Int J Equity Health. 2021 Jul 30;20(1):176. doi: 10.1186/s12939-021-01512-4. Int J Equity Health. 2021. PMID: 34330292 Free PMC article.
-
Factors Associated With Child Stunting, Wasting, and Underweight in 35 Low- and Middle-Income Countries.JAMA Netw Open. 2020 Apr 1;3(4):e203386. doi: 10.1001/jamanetworkopen.2020.3386. JAMA Netw Open. 2020. PMID: 32320037 Free PMC article.
-
Intersectional Inequalities in Anthropometric Failure among Indian Children: Evidence from the National Family Health Survey (2015-2016).J Biosoc Sci. 2023 Jul;55(4):669-696. doi: 10.1017/S0021932022000323. Epub 2022 Oct 4. J Biosoc Sci. 2023. PMID: 36193705
-
Wealth-based disparities in the prevalence of short birth interval in India: insights from NFHS-5.Popul Health Metr. 2024 Jul 11;22(1):14. doi: 10.1186/s12963-024-00334-0. Popul Health Metr. 2024. PMID: 38992717 Free PMC article.
Cited by
-
Decomposing social groups differential in stunting among children under five in India using nationally representative sample data.Sci Rep. 2024 Nov 8;14(1):27260. doi: 10.1038/s41598-024-78796-3. Sci Rep. 2024. PMID: 39516279 Free PMC article.
-
An evolution of inequality of opportunity in the nutritional outcomes of under-five children in Malawi.SSM Popul Health. 2024 Jan 12;25:101606. doi: 10.1016/j.ssmph.2024.101606. eCollection 2024 Mar. SSM Popul Health. 2024. PMID: 38292048 Free PMC article.
-
Trends in socioeconomic inequality in mortality during childhood between 1993 and 2021 in India.BMJ Glob Health. 2025 May 2;10(5):e016386. doi: 10.1136/bmjgh-2024-016386. BMJ Glob Health. 2025. PMID: 40316411 Free PMC article.
References
-
- Black R.E., Victora C.G., Walker S.P., Bhutta Z.A., Christian P., de Onis M., Ezzati M., Grantham-McGregor S., Katz J., Martorell R., Uauy R. Maternal and child undernutrition and overweight in low-income and middle-income countries. The Lancet. 2013;382(9890):427–451. doi: 10.1016/S0140-6736(13)60937-X. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
