

Clinical Characteristics of Tracheobronchopathia Osteochondroplastica: A Retrospective Study of 33 Patients
- PMID: 37601808
- PMCID: PMC10438451
- DOI: 10.2147/IJGM.S418394
Clinical Characteristics of Tracheobronchopathia Osteochondroplastica: A Retrospective Study of 33 Patients
Abstract
Introduction: Tracheobronchopathia osteochondroplastica (TO) is a relatively rare benign tracheobronchial disease, which is often misdiagnosed or missed. To date, there is no specific treatment for TO. The aim of this study was to investigate the clinical manifestations, imaging features, bronchoscopy results, pathological findings, and diagnostic points of TO.
Patients and methods: A total of 33 patients diagnosed with TO were enrolled. Clinical data were collected using retrospective methods in the period from January 2021 and November 2022. Descriptive analysis was used.
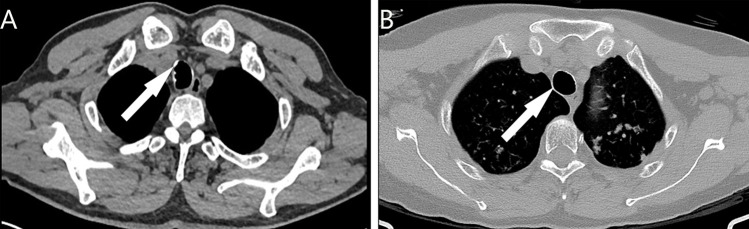
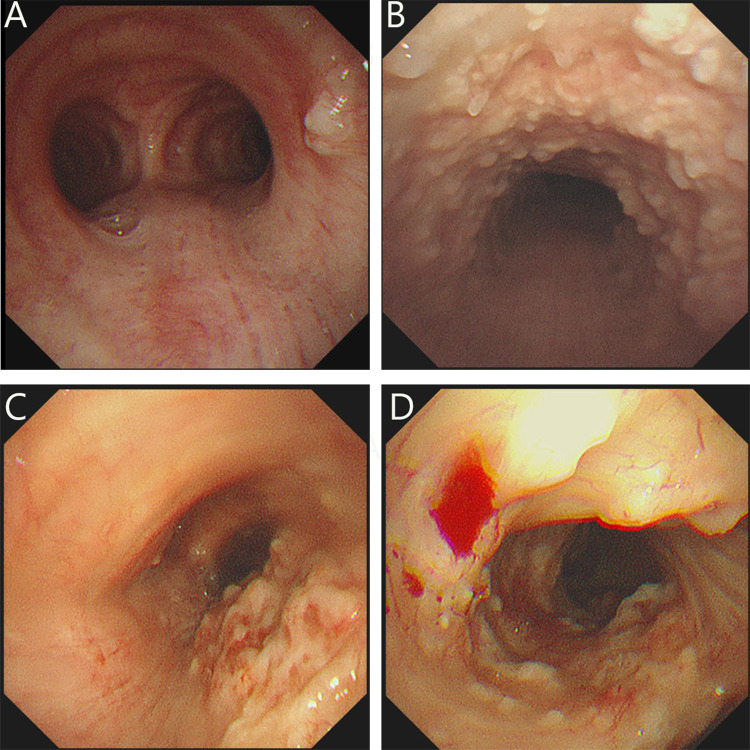
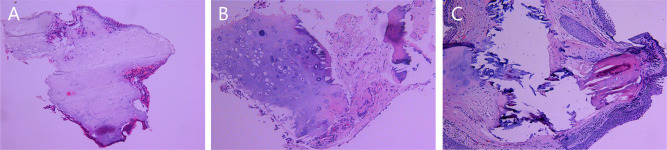
Results: Patients included 17 (51.5%) male and 16 (48.5%) female, with a median age of 54 years. The main clinical manifestations included cough in 15 cases, fever in 6 cases, chest tightness in 4 cases, haemoptysis in 3 cases, and chest pain in 4 cases. The time from the onset of symptoms to diagnosis was 1 week to 96 months. Some patients were diagnosed with other lung diseases, including 16 patients with tuberculosis, 2 patients with lung cancer, 3 patients with nontuberculous mycobacteriosis, 3 patients with tuberculous pleurisy, 2 patients with bronchiectasis, and 1 patient with pneumonia. Chest computed tomography (CT) scan demonstrated calcified nodules in 10 (30.3%) patients. In bronchoscopy, entire tracheal involvement was found in 21 (63.6%) patients, 12 (36.4%) patients were found to have involvement of only part of the trachea. The patients were divided into three groups according to the bronchoscopic presentation, the largest proportion was stage II (19/33), followed by stage I (8/33) and stage III (6/33). Histopathological findings showed squamous metaplasia, cartilaginous, and bony tissues.
Conclusion: TO is a slowly progressing disease with non-specific clinical symptoms and a low positive rate of imaging diagnosis, making it susceptible to misdiagnosis and missed diagnosis. The disease needs to be diagnosed by combining imaging features, fiberoptic bronchoscopy, and pathological findings.
Keywords: benign tracheobronchial disease; bronchoscopy; misdiagnosis; tuberculosis.
© 2023 Liu et al.
Conflict of interest statement
The authors have no conflicts of interest to declare for this work.
Figures
References
LinkOut - more resources
Full Text Sources
