

Central hyperthyroidism combined with Graves' disease: case series and review of the literature
- PMID: 37602950
- PMCID: PMC10388650
- DOI: 10.1530/ETJ-22-0223
Central hyperthyroidism combined with Graves' disease: case series and review of the literature
Abstract
Background: Central hyperthyroidism is characterized by elevated free thyroid hormone and unsuppressed thyroid-stimulating hormone (TSH), and this laboratory feature includes TSH-secreting pituitary adenoma (TSHoma) and resistance to thyroid hormone β (RTHβ). Central hyperthyroidism combined with Graves' disease (GD) has been rarely reported.
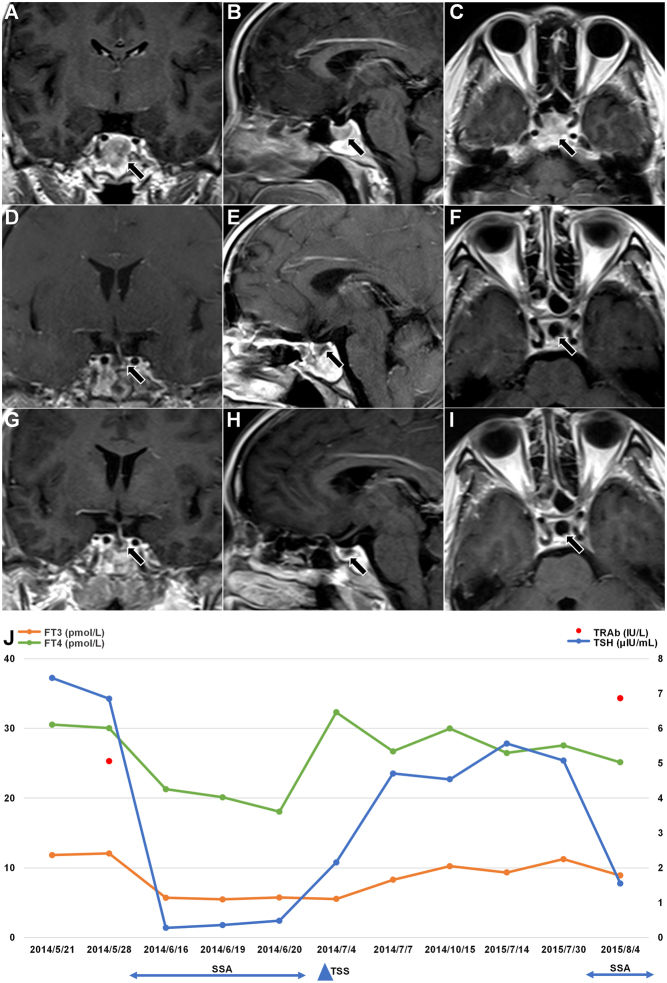
Case report: We describe three patients with TSHoma combined with GD and one patient with GD combined with RTHβ and pituitary adenoma. These three patients with TSHoma combined with GD showed elevated thyroid hormone, while TSH level was normal or elevated, and TSH receptor antibodies were positive. After thyrotoxicosis was controlled, they all underwent transsphenoidal surgery. We also describe a patient with an initial presentation of GD who developed hypothyroidism after anti-hyperthyroidism treatment and TSH was inappropriately significantly increased. His head magnetic resonance imaging revealed a pituitary adenoma. Genetic testing confirmed a heterozygous mutation in the thyroid hormone receptor β gene c.1148G>A (p.R383H). After levothyroxine and desiccated thyroid tablet treatment, the TSH level decreased to normal.
Conclusion: These four cases highlight the need to consider the diagnosis of GD combined with central hyperthyroidism when faced with inconsistent thyroid function test results, illuminating the specific diagnostic and therapeutic challenges of coexisting primary and central hyperthyroidism. Finally, we propose clinical management for central hyperthyroidism combined with GD.
Keywords: Graves’ disease; central hyperthyroidism; resistance to thyroid hormone β; thyroid-stimulating hormone-secreting pituitary adenoma.
Conflict of interest statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of this review.
Figures




Similar articles
-
Concurrent Graves' Disease and TSH Secreting Pituitary Adenoma Presenting Suppressed Thyrotropin Levels: A Case Report and Review of the Literature.Front Endocrinol (Lausanne). 2020 Aug 6;11:523. doi: 10.3389/fendo.2020.00523. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32849306 Free PMC article. Review.
-
Thyrotropin-producing pituitary adenoma simultaneously existing with Graves' disease: a case report.J Med Case Rep. 2017 Jan 6;11(1):9. doi: 10.1186/s13256-016-1172-4. J Med Case Rep. 2017. PMID: 28061802 Free PMC article.
-
A remarkable case of thyrotoxicosis initially caused by graves' disease followed by a probable TSHoma - a case report.BMC Endocr Disord. 2020 Aug 27;20(1):133. doi: 10.1186/s12902-020-00611-7. BMC Endocr Disord. 2020. PMID: 32854689 Free PMC article.
-
Coexistence of thyroid-stimulating hormone-secreting pituitary adenoma and graves' hyperthyroidism.Eur Thyroid J. 2014 Mar;3(1):60-4. doi: 10.1159/000355386. Epub 2013 Nov 20. Eur Thyroid J. 2014. PMID: 24847468 Free PMC article.
-
A challenging TSH/GH co-secreting pituitary adenoma with concomitant thyroid cancer; a case report and literature review.BMC Endocr Disord. 2021 Aug 30;21(1):177. doi: 10.1186/s12902-021-00839-x. BMC Endocr Disord. 2021. PMID: 34461869 Free PMC article. Review.
Cited by
-
Mixed thyrotropin-secreting pituitary neuroendocrine tumor coexisting with Graves' disease: a case report.Front Med (Lausanne). 2024 Sep 4;11:1436400. doi: 10.3389/fmed.2024.1436400. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39296905 Free PMC article.
-
A Rare Coexistence of Thyrotropin-Secreting Pituitary Adenoma and Graves Disease.JCEM Case Rep. 2025 Jul 31;3(9):luaf173. doi: 10.1210/jcemcr/luaf173. eCollection 2025 Sep. JCEM Case Rep. 2025. PMID: 40746500 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
