

Effect of Bypassing the Closest Stroke Center in Patients with Intracerebral Hemorrhage: A Secondary Analysis of the RACECAT Randomized Clinical Trial
- PMID: 37603325
- PMCID: PMC10442788
- DOI: 10.1001/jamaneurol.2023.2754
Effect of Bypassing the Closest Stroke Center in Patients with Intracerebral Hemorrhage: A Secondary Analysis of the RACECAT Randomized Clinical Trial
Abstract
Importance: Prehospital transfer protocols are based on rapid access to reperfusion therapies for patients with ischemic stroke. The effect of different protocols among patients receiving a final diagnosis of intracerebral hemorrhage (ICH) is unknown.
Objective: To determine the effect of direct transport to an endovascular treatment (EVT)-capable stroke center vs transport to the nearest local stroke center.
Design, setting, and participants: This was a prespecified secondary analysis of RACECAT, a multicenter, population-based, cluster-randomized clinical trial conducted from March 2017 to June 2020 in Catalonia, Spain. Patients were evaluated by a blinded end point assessment. All consecutive patients suspected of experiencing a large vessel occlusion stroke (Rapid Arterial Occlusion Evaluation Scale [RACE] score in the field >4 on a scale of 0 to 9, with lower to higher stroke severity) with final diagnosis of ICH were included. A total of 1401 patients were enrolled in RACECAT with suspicion of large vessel occlusion stroke. The current analysis was conducted in October 2022.
Intervention: Direct transport to an EVT-capable stroke center (n = 137) or to the closest local stroke center (n = 165).
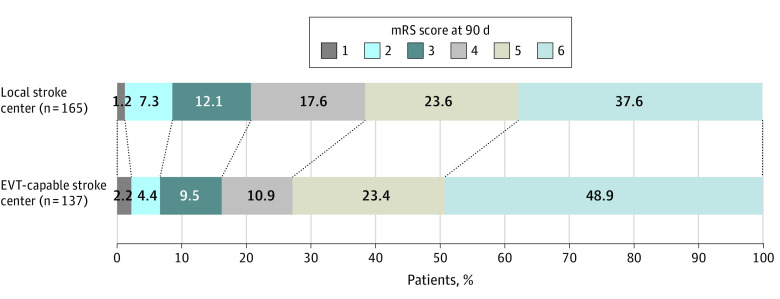
Main outcomes and measures: The primary outcome was tested using cumulative ordinal logistic regression to estimate the common odds ratio (OR) and 95% CI of the shift analysis of disability at 90 days as assessed by the modified Rankin Scale (mRS) score (range, 0 [no symptoms] to 6 [death]) in the intention-to-treat population. Secondary outcomes, included 90-day mortality, death or severe functional dependency, early neurological deterioration, early mortality, ICH volume and enlargement, rate of neurosurgical treatment, rate of clinical complications during initial transport, and rate of adverse events until day 5.
Results: Of 1401 patients enrolled, 1099 were excluded from this analysis (32 rejected informed consent, 920 had ischemic stroke, 29 had transient ischemic attack, 12 had subarachnoid hemorrhage, and 106 had stroke mimic). Thus, 302 patients were included (204 [67.5%] men; mean [SD] age 71.7 [12.8] years; and median [IQR] RACE score, 7 [6-8]). For the primary outcome, direct transfer to an EVT-capable stroke center (mean [SD] mRS score, 4.93 [1.38]) resulted in worse functional outcome at 90 days compared with transfer to the nearest local stroke center (mean [SD] mRS score, 4.66 [1.39]; adjusted common OR, 0.63; 95% CI, 0.41-0.96). Direct transfer to an EVT-capable stroke center also suggested potentially higher 90-day mortality compared with transfer to the nearest local stroke center (67 of 137 [48.9%] vs 62 of 165 [37.6%]; adjusted hazard ratio, 1.40; 95% CI, 0.99-1.99). The rates of medical complications during the initial transfer (30 of 137 [22.6%] vs 9 of 165 patients [5.6%]; adjusted OR, 5.29; 95% CI, 2.38-11.73) and in-hospital pneumonia (49 of 137 patients [35.8%] vs 29 of 165 patients [17.6%]; OR, 2.61; 95% CI, 1.53-4.44) were higher in the EVT-capable stroke center group.
Conclusions and relevance: In this secondary analysis of the RACECAT randomized clinical trial, bypassing the closest stroke center resulted in reduced chances of functional independence at 90 days for patients who received a final diagnosis of ICH.
Trial registration: ClinicalTrials.gov Identifier: NCT02795962.
Conflict of interest statement
Figures


Comment in
- doi: 10.1001/jamaneurol.2023.2753
References
-
- van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9(2):167-176. doi:10.1016/S1474-4422(09)70340-0 - DOI - PubMed
-
- Greenberg SM, Ziai WC, Cordonnier C, et al. . 2022 Guideline for the management of patients with spontaneous intracerebral hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke. 2022; 53(7):e282-e361. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
