

Late Mortality After COVID-19 Infection Among US Veterans vs Risk-Matched Comparators: A 2-Year Cohort Analysis
- PMID: 37603339
- PMCID: PMC10442778
- DOI: 10.1001/jamainternmed.2023.3587
Late Mortality After COVID-19 Infection Among US Veterans vs Risk-Matched Comparators: A 2-Year Cohort Analysis
Erratum in
-
Error in Nonauthor Collaborator Supplement.JAMA Intern Med. 2024 Apr 1;184(4):453. doi: 10.1001/jamainternmed.2023.8594. JAMA Intern Med. 2024. PMID: 38315461 Free PMC article. No abstract available.
Abstract
Importance: Despite growing evidence of persistent problems after acute COVID-19, how long the excess mortality risk associated with COVID-19 persists is unknown.
Objective: To measure the time course of differential mortality among Veterans who had a first-documented COVID-19 infection by separately assessing acute mortality from later mortality among matched groups with infected and uninfected individuals who survived and were uncensored at the start of each period.
Design, settings, and participants: This retrospective cohort study used prospectively collected health record data from Veterans Affairs hospitals across the US on Veterans who had COVID-19 between March 2020 and April 2021. Each individual was matched with up to 5 comparators who had not been infected with COVID-19 at the time of matching. This match balanced, on a month-by-month basis, the risk of developing COVID-19 using 37 variables measured in the 24 months before the date of the infection or match. A primary analysis censored comparators when they developed COVID-19 with inverse probability of censoring weighting in Cox regression. A secondary analysis did not censor. Data analyses were performed from April 2021 through June 2023.
Exposure: First-documented case of COVID-19 (SARS-CoV-2) infection.
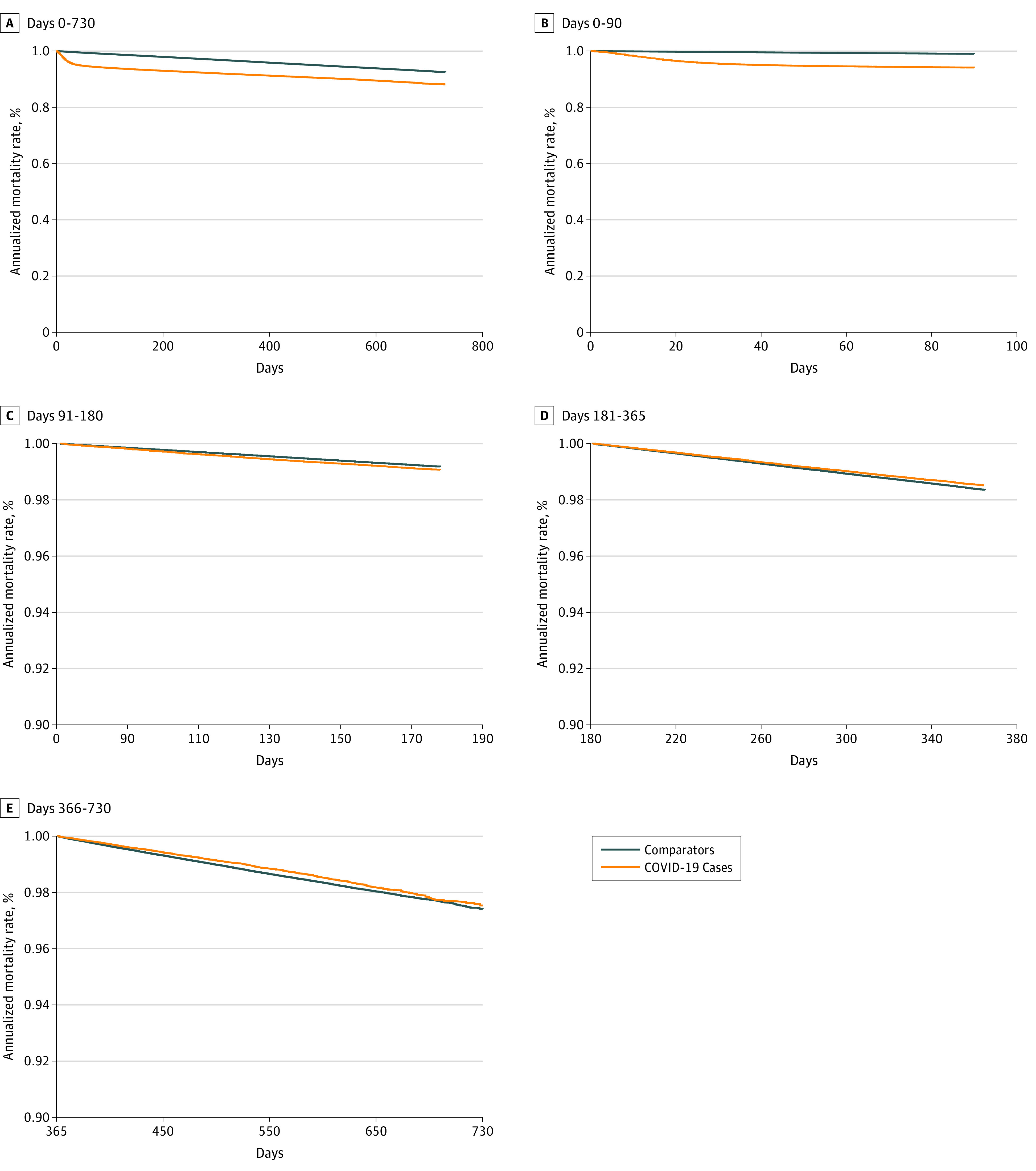
Main outcome measures: Hazard ratios for all-cause mortality at clinically meaningful intervals after infection: 0 to 90, 91 to 180, 181 to 365, and 366 to 730 days.
Results: The study sample comprised 208 061 Veterans with first-documented COVID-19 infection (mean [SD] age, 60.5 (16.2) years; 21 936 (10.5) women; 47 645 [22.9] Black and 139 604 [67.1] White individuals) and 1 037 423 matched uninfected comparators with similar characteristics. Veterans with COVID-19 had an unadjusted mortality rate of 8.7% during the 2-year period after the initial infection compared with 4.1% among uninfected comparators, with censoring if the comparator later developed COVID-19-an adjusted hazard ratio (aHR) of 2.01 (95% CI, 1.98-2.04). The risk of excess death varied, being highest during days 0 to 90 after infection (aHR, 6.36; 95% CI, 6.20-6.51) and still elevated during days 91 to 180 (aHR, 1.18; 95% CI, 1.12-1.23). Those who survived COVID-19 had decreased mortality on days 181 to 365 (aHR, 0.92; 95% CI, 0.89-0.95) and 366 to 730 (aHR, 0.89; 95% CI, 0.85-0.92). These patterns were consistent across sensitivity analyses.
Conclusion and relevance: The findings of this retrospective cohort study indicate that although overall 2-year mortality risk was worse among those infected with COVID-19, by day 180 after infection they had no excess mortality during the next 1.5 years.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
