

Ancestry-based differences in the immune phenotype are associated with lupus activity
- PMID: 37606045
- PMCID: PMC10543734
- DOI: 10.1172/jci.insight.169584
Ancestry-based differences in the immune phenotype are associated with lupus activity
Abstract
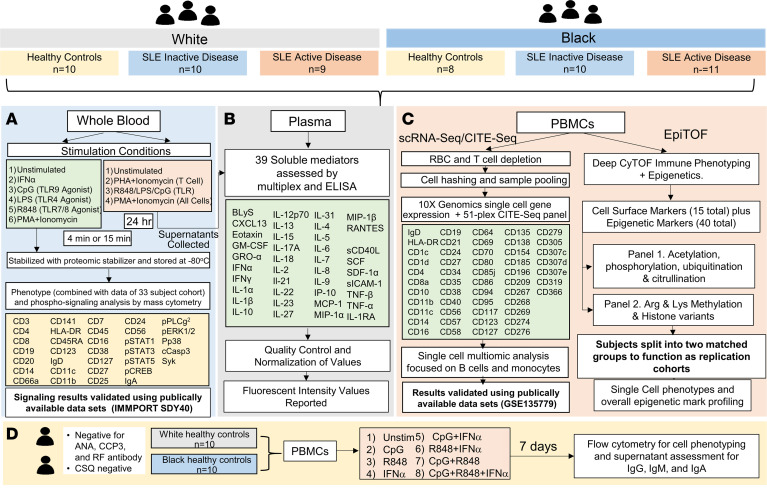
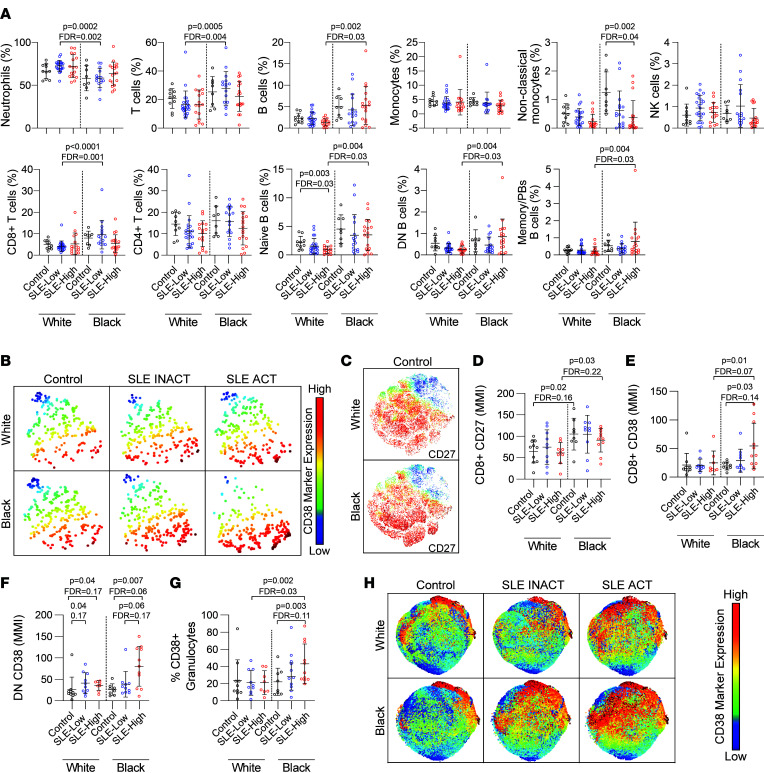
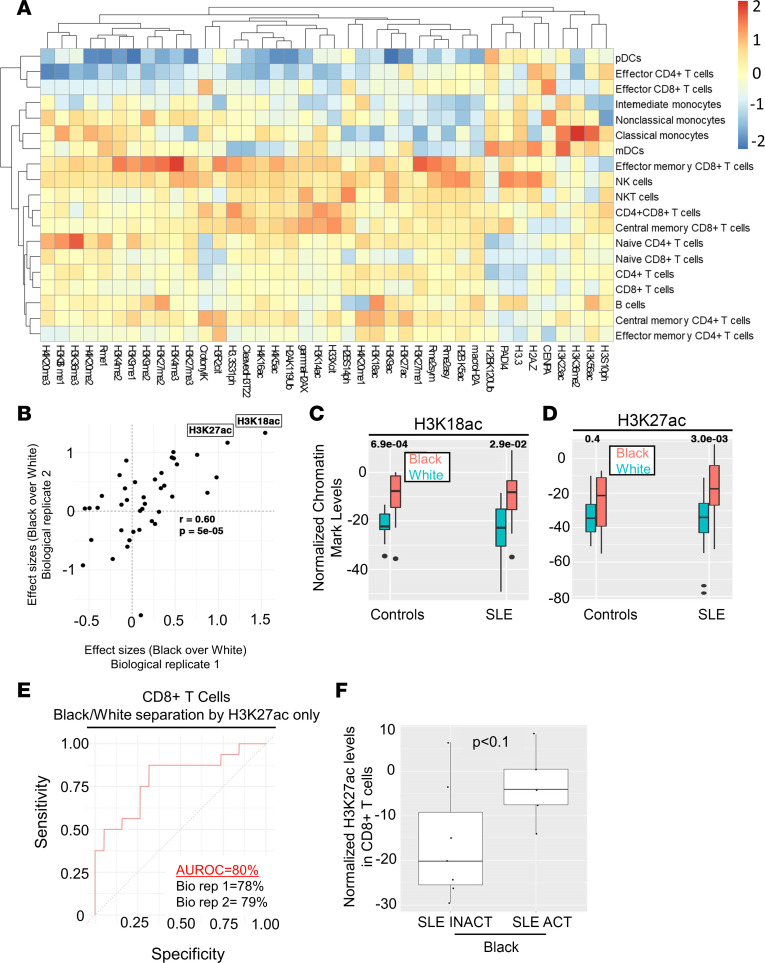
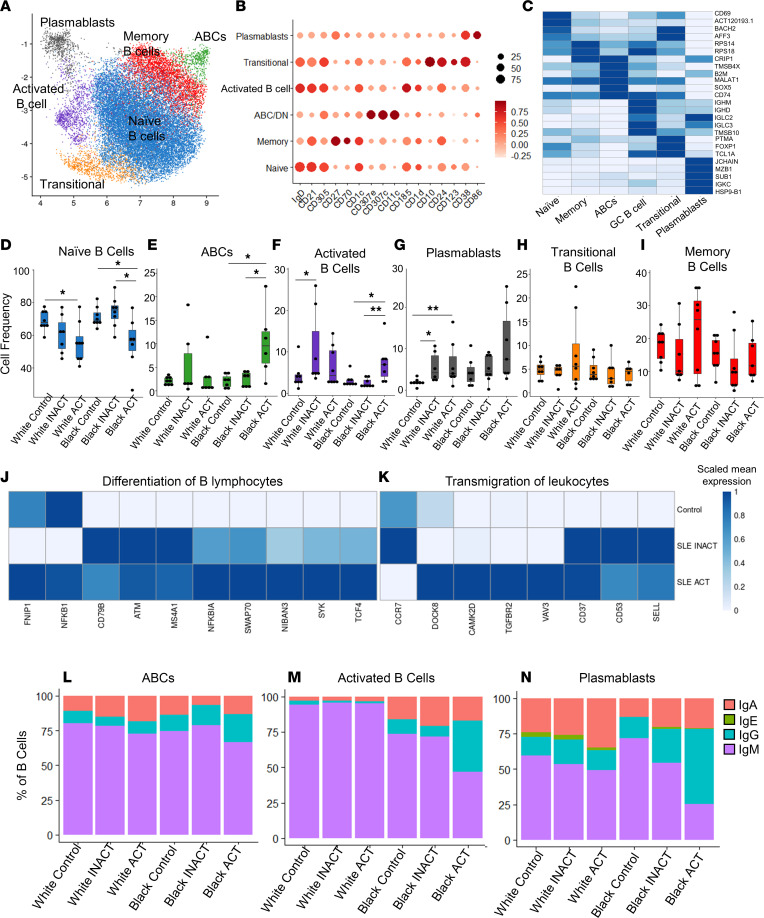
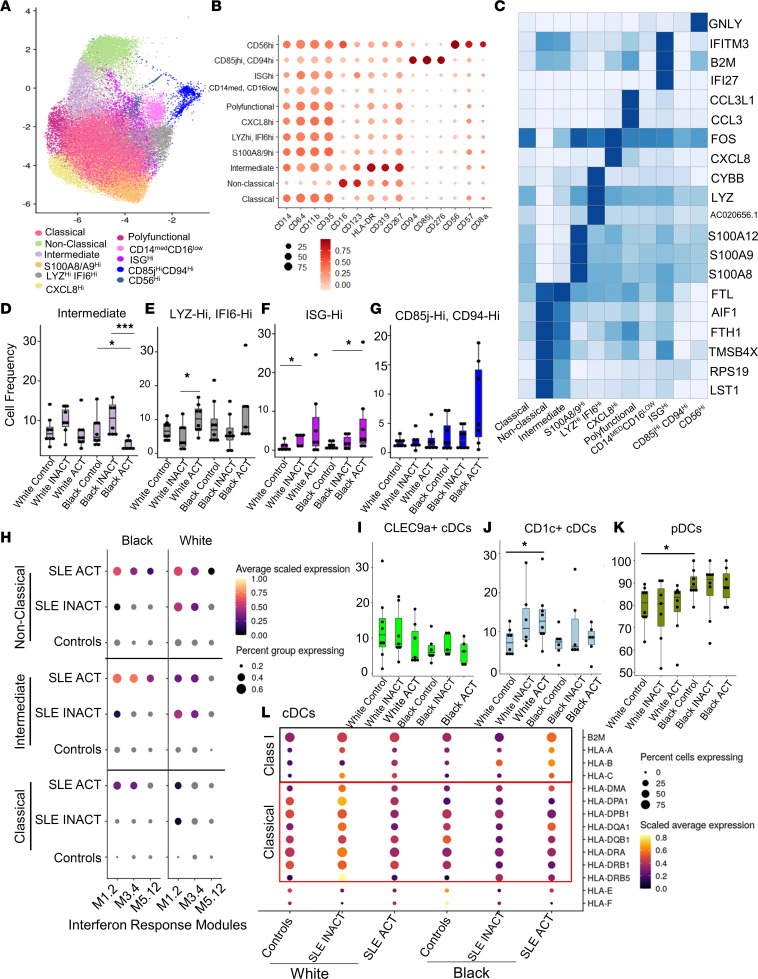
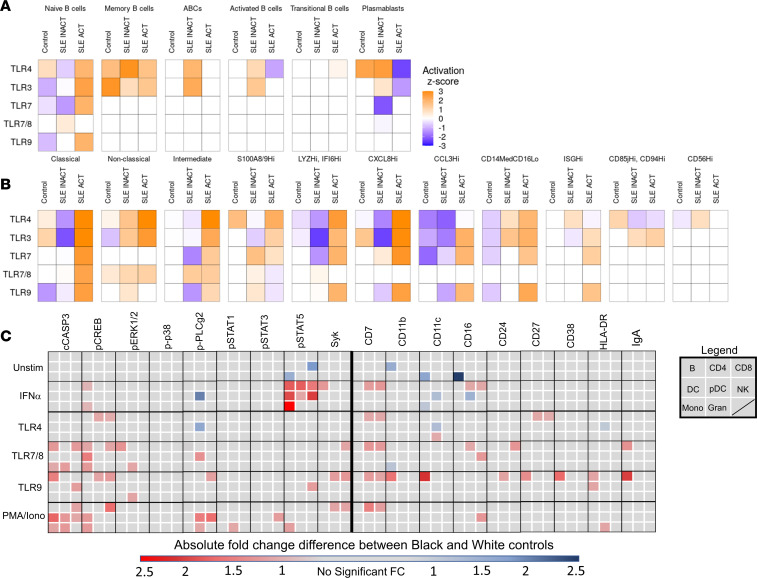
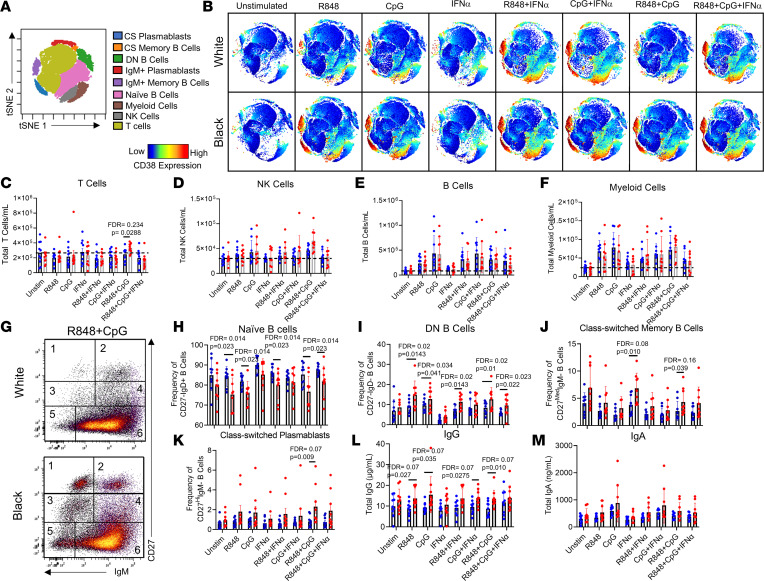
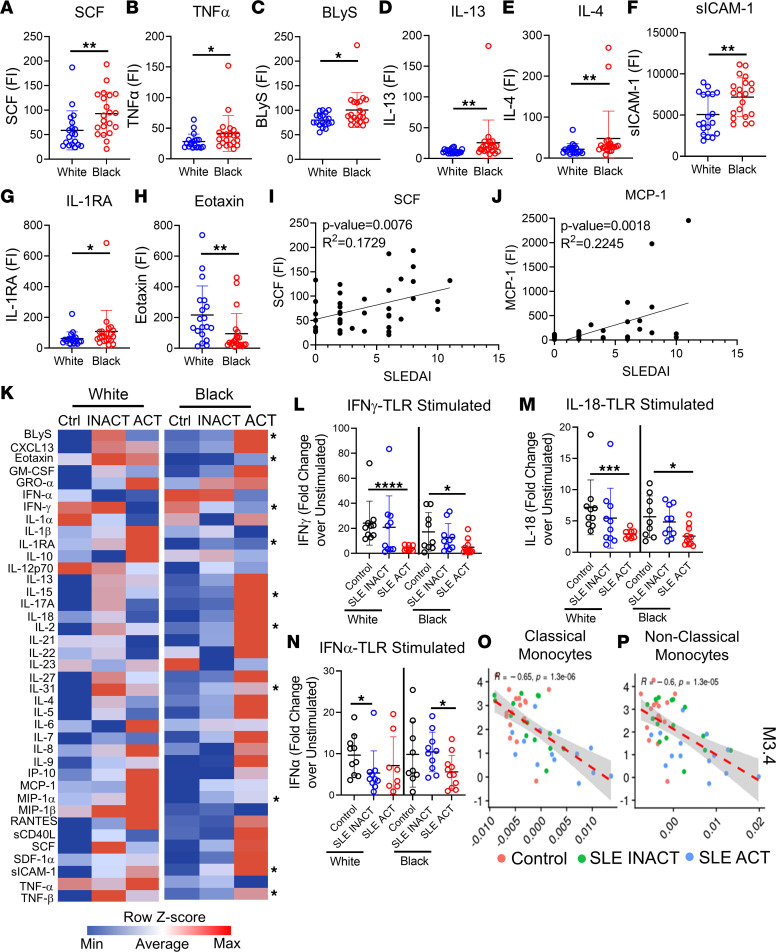
Systemic lupus erythematosus (SLE) affects 1 in 537 Black women, which is >2-fold more than White women. Black patients develop the disease at a younger age, have more severe symptoms, and have a greater chance of early mortality. We used a multiomics approach to uncover ancestry-associated immune alterations in patients with SLE and healthy controls that may contribute biologically to disease disparities. Cell composition, signaling, epigenetics, and proteomics were evaluated by mass cytometry; droplet-based single-cell transcriptomics and proteomics; and bead-based multiplex soluble mediator levels in plasma. We observed altered whole blood frequencies and enhanced activity in CD8+ T cells, B cells, monocytes, and DCs in Black patients with more active disease. Epigenetic modifications in CD8+ T cells (H3K27ac) could distinguish disease activity level in Black patients and differentiate Black from White patient samples. TLR3/4/7/8/9-related gene expression was elevated in immune cells from Black patients with SLE, and TLR7/8/9 and IFN-α phospho-signaling and cytokine responses were heightened even in immune cells from healthy Black control patients compared with White individuals. TLR stimulation of healthy immune cells recapitulated the ancestry-associated SLE immunophenotypes. This multiomic resource defines ancestry-associated immune phenotypes that differ between Black and White patients with SLE, which may influence the course and severity of SLE and other diseases.
Keywords: Autoimmunity; Cytokines; Immunology; Lupus; Signal transduction.
Figures
References
-
- Lewis MJ, Jawad AS. The effect of ethnicity and genetic ancestry on the epidemiology, clinical features and outcome of systemic lupus erythematosus. Rheumatology (Oxford) 2017;56(suppl 1):67–i77. - PubMed
-
- Alarcon GS, et al. Systemic lupus erythematosus in three ethnic groups: II. Features predictive of disease activity early in its course. LUMINA Study Group. Lupus in minority populations, nature versus nurture. Arthritis Rheum. 1998;41(7):1173–1180. doi: 10.1002/1529-0131(199807)41:7<1173::AID-ART5>3.0.CO;2-A. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
