

Regorafenib plus Vincristine and Irinotecan in Pediatric Patients with Recurrent/Refractory Solid Tumors: An Innovative Therapy for Children with Cancer Study
- PMID: 37606641
- PMCID: PMC10618645
- DOI: 10.1158/1078-0432.CCR-23-0257
Regorafenib plus Vincristine and Irinotecan in Pediatric Patients with Recurrent/Refractory Solid Tumors: An Innovative Therapy for Children with Cancer Study
Abstract
Purpose: This phase Ib study defined the safety, MTD, and recommended phase II dose (RP2D) of regorafenib combined with vincristine and irinotecan (VI). Secondary objectives were evaluation of antitumor activity and pharmacokinetics (PK) of regorafenib and irinotecan.
Patients and methods: Patients aged 6 months to <18 years with relapsed/refractory solid malignancies [≥50% with rhabdomyosarcoma (RMS)] received regorafenib (starting dose 72 mg/m2/day) concomitantly or sequentially with vincristine 1.5 mg/m2 on days 1 and 8, and irinotecan 50 mg/m2 on days 1-5 (21-day cycle). Adverse events (AE) and tumor response were assessed. PK (regorafenib and irinotecan) were evaluated using a population PK model.
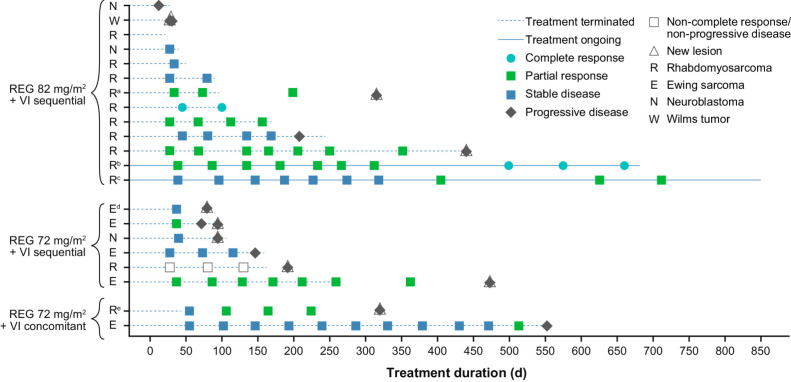
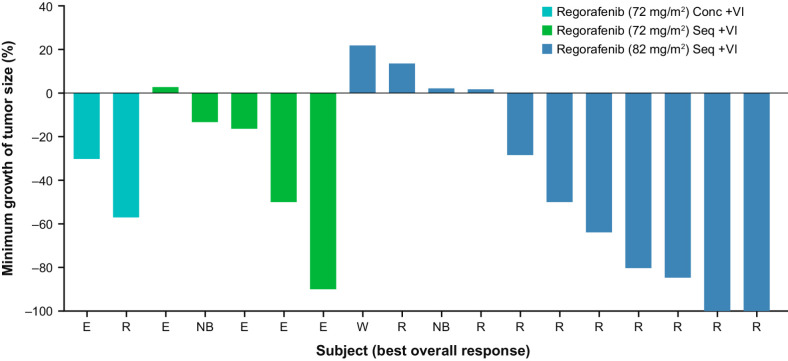
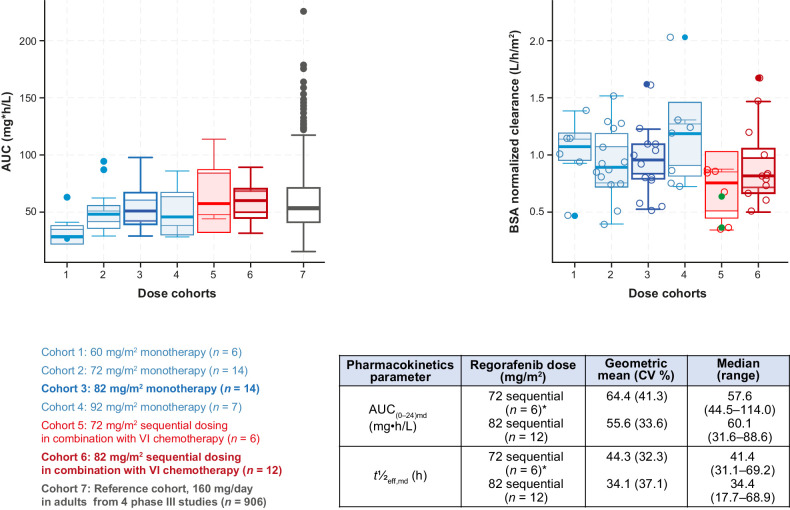
Results: We enrolled 21 patients [median age, 10 years; 12, RMS; 5, Ewing sarcoma (EWS)]. The MTD/RP2D of regorafenib in the sequential schedule was 82 mg/m2. The concomitant dosing schedule was discontinued because of dose-limiting toxicities in 2 of 2 patients treated. Most common grade 3/4 (>30% of patients) AEs were neutropenia, anemia, thrombocytopenia, and leukopenia. The overall response rate was 48% and disease control rate [complete response (CR)/partial response/stable disease/non-CR/non-progressive disease] was 86%. Median progression-free survival was 7.0 months [95% confidence interval (CI), 2.9-14.8] and median overall survival was 8.7 months (95% CI, 5.5-16.3). When combined with VI, regorafenib PK was similar to single-agent PK in children and adults (treated with regorafenib 160 mg/day).
Conclusions: Regorafenib can be combined sequentially with standard dose VI in pediatric patients with relapsed/refractory solid tumors with appropriate dose modifications. Clinical activity was observed in patients with RMS and EWS (ClinicalTrials.gov NCT02085148).
©2023 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- US Food and Drug Administration. Stivarga (regorafenib) prescribing information. Bayer HealthCare Pharmaceuticals, Whippany, NJ, USA. 2020. Available from: https://labeling.bayerhealthcare.com/html/products/pi/Stivarga_PI.pdf.
-
- European Medicines Agency. Stivarga (regorafenib) summary of product characteristics. Bayer AG, Leverkusen, Germany. 2023. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/stivarga#product-infor....
-
- Wilhelm SM, Dumas J, Adnane L, Lynch M, Carter CA, Schutz G, et al. Regorafenib (BAY 73–4506): a new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int J Cancer 2011;129:245–55. - PubMed
-
- Abou-Elkacem L, Arns S, Brix G, Gremse F, Zopf D, Kiessling F, et al. Regorafenib inhibits growth, angiogenesis, and metastasis in a highly aggressive, orthotopic colon cancer model. Mol Cancer Ther 2013;12:1322–31. - PubMed
-
- Chan AS, Leung SY, Wong MP, Yuen ST, Cheung N, Fan YW, et al. Expression of vascular endothelial growth factor and its receptors in the anaplastic progression of astrocytoma, oligodendroglioma, and ependymoma. Am J Surg Pathol 1998;22:816–26. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
