

Evaluation of Large-Scale Proteomics for Prediction of Cardiovascular Events
- PMID: 37606673
- PMCID: PMC10445198
- DOI: 10.1001/jama.2023.13258
Evaluation of Large-Scale Proteomics for Prediction of Cardiovascular Events
Abstract
Importance: Whether protein risk scores derived from a single plasma sample could be useful for risk assessment for atherosclerotic cardiovascular disease (ASCVD), in conjunction with clinical risk factors and polygenic risk scores, is uncertain.
Objective: To develop protein risk scores for ASCVD risk prediction and compare them to clinical risk factors and polygenic risk scores in primary and secondary event populations.
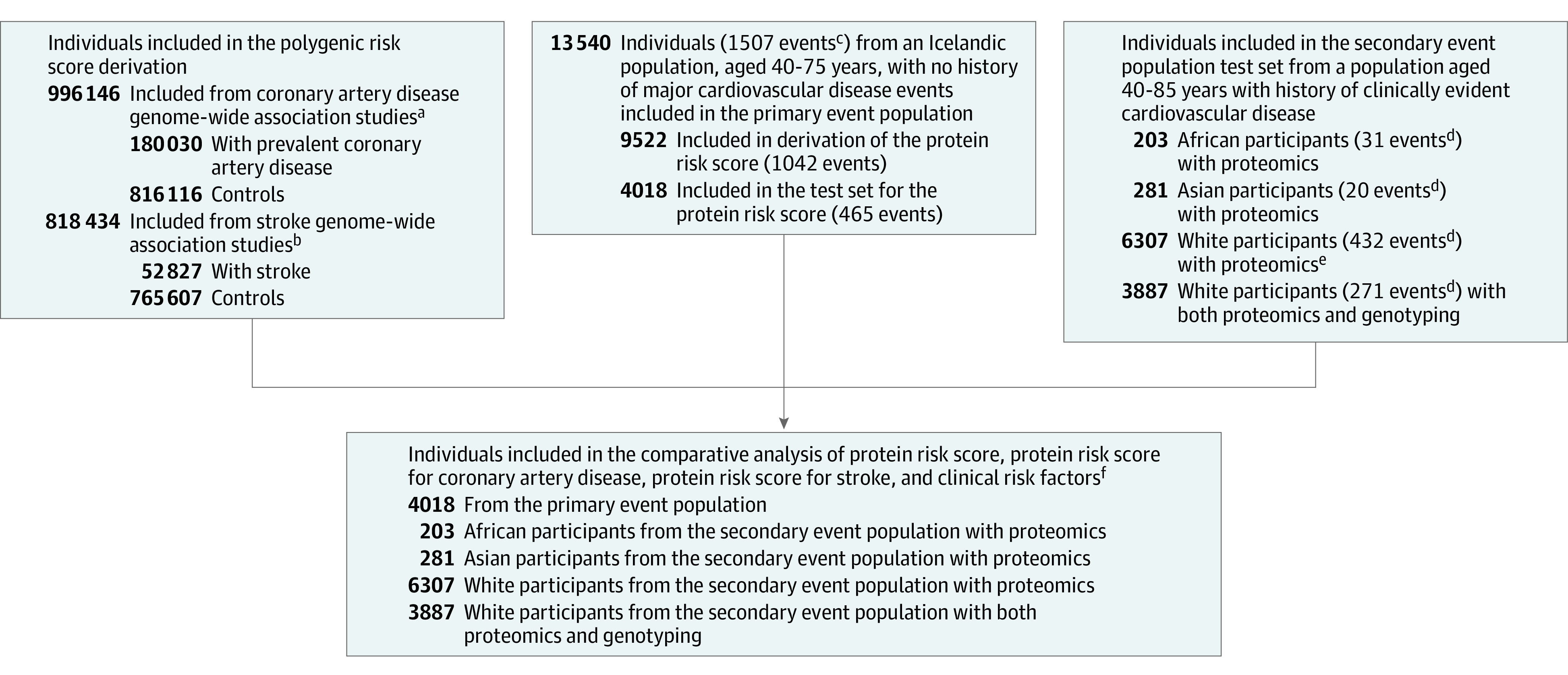
Design, setting, and participants: The primary analysis was a retrospective study of primary events among 13 540 individuals in Iceland (aged 40-75 years) with proteomics data and no history of major ASCVD events at recruitment (study duration, August 23, 2000 until October 26, 2006; follow-up through 2018). We also analyzed a secondary event population from a randomized, double-blind lipid-lowering clinical trial (2013-2016), consisting of individuals with stable ASCVD receiving statin therapy and for whom proteomic data were available for 6791 individuals.
Exposures: Protein risk scores (based on 4963 plasma protein levels and developed in a training set in the primary event population); polygenic risk scores for coronary artery disease and stroke; and clinical risk factors that included age, sex, statin use, hypertension treatment, type 2 diabetes, body mass index, and smoking status at the time of plasma sampling.
Main outcomes and measures: Outcomes were composites of myocardial infarction, stroke, and coronary heart disease death or cardiovascular death. Performance was evaluated using Cox survival models and measures of discrimination and reclassification that accounted for the competing risk of non-ASCVD death.
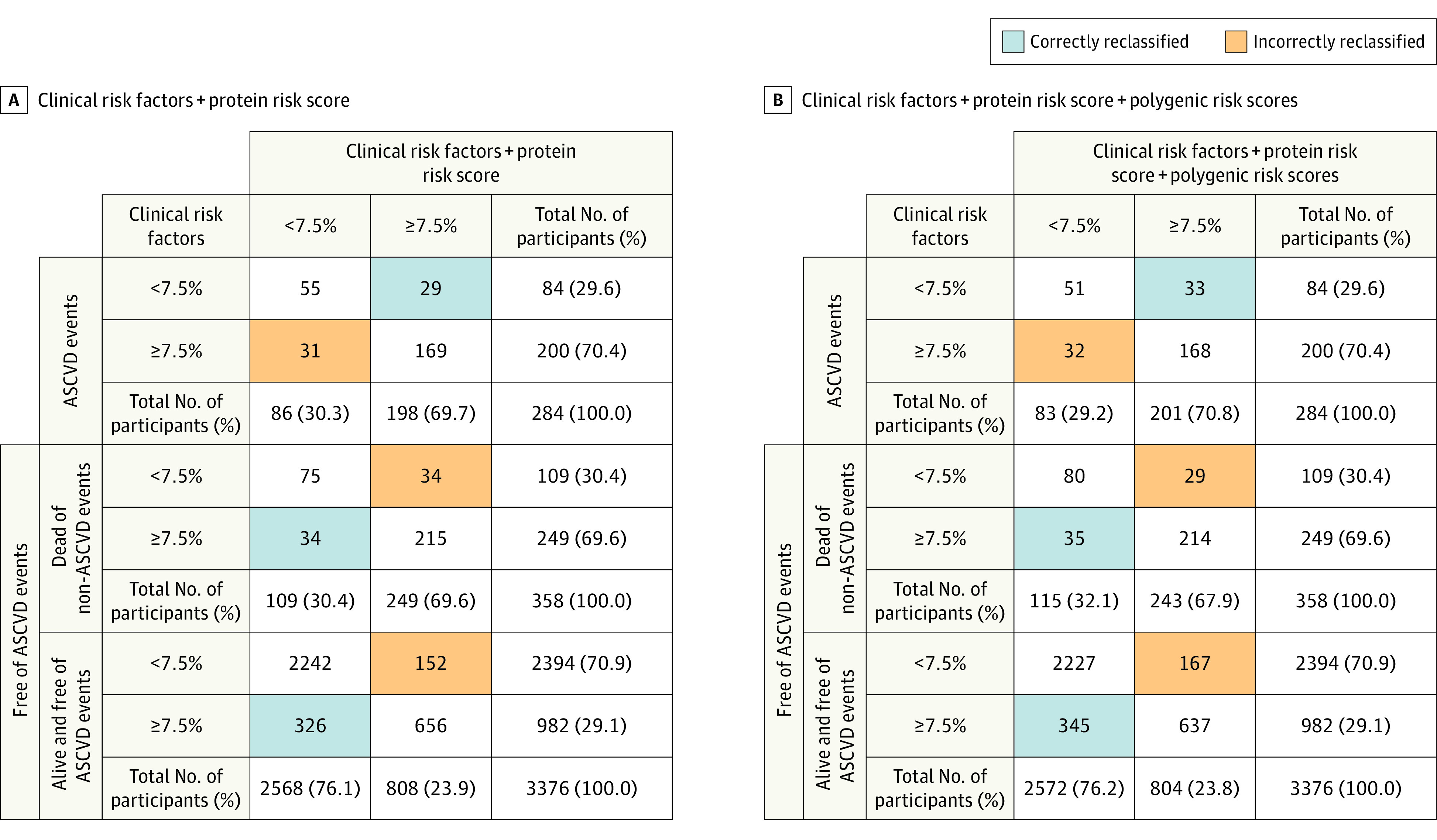
Results: In the primary event population test set (4018 individuals [59.0% women]; 465 events; median follow-up, 15.8 years), the protein risk score had a hazard ratio (HR) of 1.93 per SD (95% CI, 1.75 to 2.13). Addition of protein risk score and polygenic risk scores significantly increased the C index when added to a clinical risk factor model (C index change, 0.022 [95% CI, 0.007 to 0.038]). Addition of the protein risk score alone to a clinical risk factor model also led to a significantly increased C index (difference, 0.014 [95% CI, 0.002 to 0.028]). Among White individuals in the secondary event population (6307 participants; 432 events; median follow-up, 2.2 years), the protein risk score had an HR of 1.62 per SD (95% CI, 1.48 to 1.79) and significantly increased C index when added to a clinical risk factor model (C index change, 0.026 [95% CI, 0.011 to 0.042]). The protein risk score was significantly associated with major adverse cardiovascular events among individuals of African and Asian ancestries in the secondary event population.
Conclusions and relevance: A protein risk score was significantly associated with ASCVD events in primary and secondary event populations. When added to clinical risk factors, the protein risk score and polygenic risk score both provided statistically significant but modest improvement in discrimination.
Conflict of interest statement
Figures
References
-
- Goff DC Jr, Lloyd-Jones DM, Bennett G, et al. ; American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25)(suppl 2):S49-S73. doi:10.1161/01.cir.0000437741.48606.98 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
