

The impact of the COVID-19 pandemic on community prescription of opioid and antineuropathic analgesics for cancer patients in Wales, UK
- PMID: 37606853
- PMCID: PMC10444652
- DOI: 10.1007/s00520-023-07944-8
The impact of the COVID-19 pandemic on community prescription of opioid and antineuropathic analgesics for cancer patients in Wales, UK
Abstract
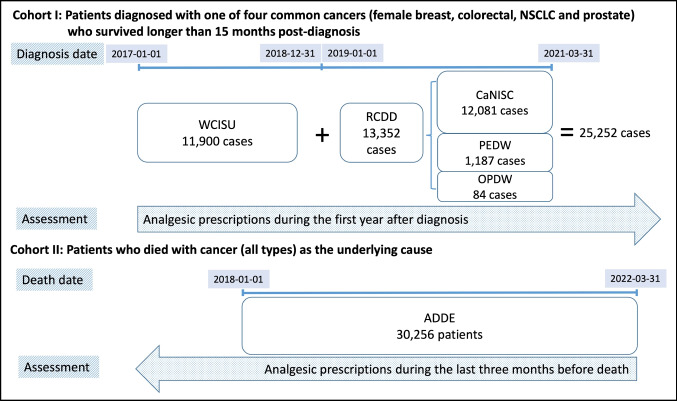
Purpose: Public health measures instituted at the onset of the COVID-19 pandemic in the UK in 2020 had profound effects on the cancer patient pathway. We hypothesise that this may have affected analgesic prescriptions for cancer patients in primary care.
Methods: A whole-nation retrospective, observational study of opioid and antineuropathic analgesics prescribed in primary care for two cohorts of cancer patients in Wales, using linked anonymised data to evaluate the impact of the pandemic and variation between different demographic backgrounds.
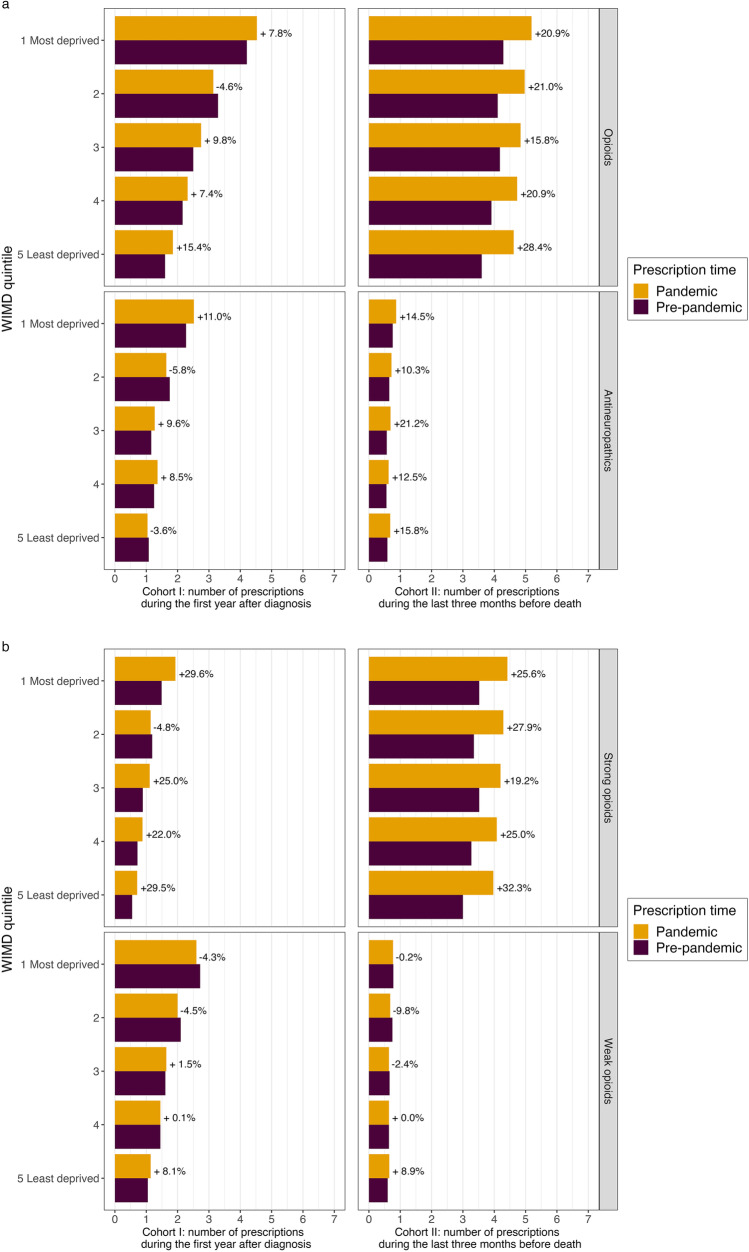
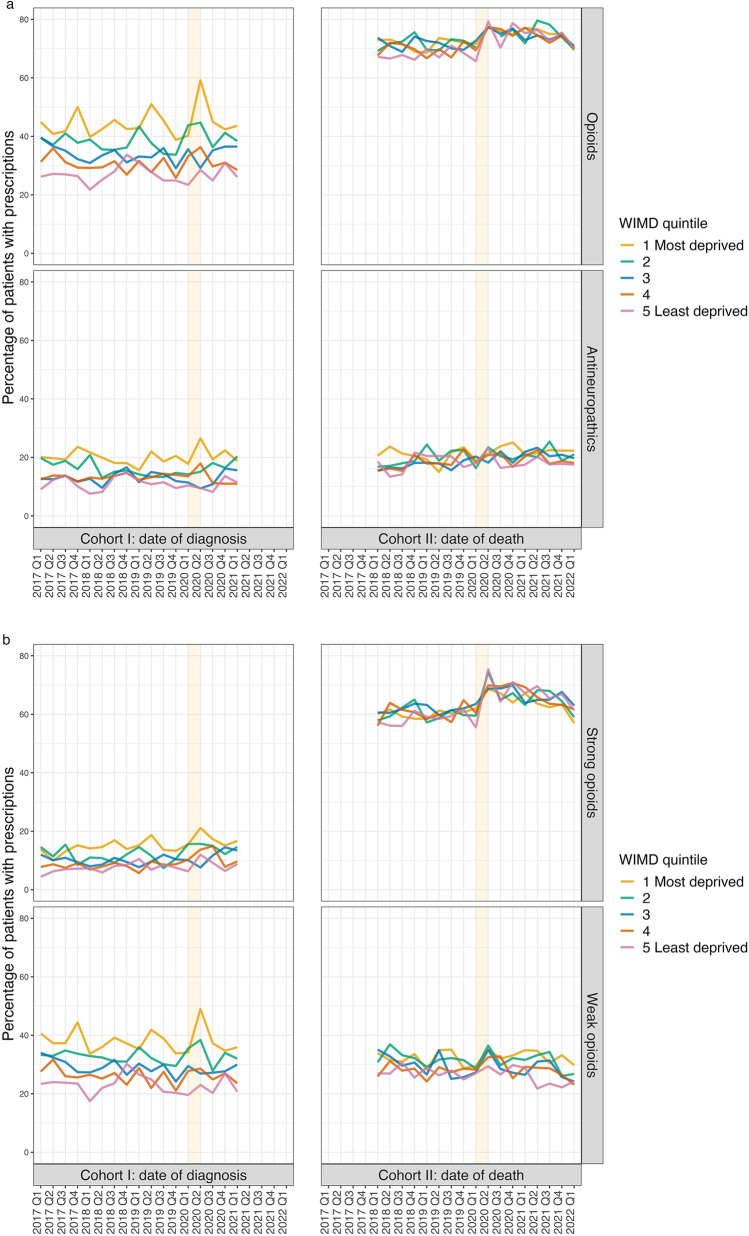
Results: We found a significant increase in strong opioid prescriptions during the pandemic for patients within their first 12 months of diagnosis with a common cancer (incidence rate ratio (IRR) 1.15, 95% CI: 1.12-1.18, p < 0.001 for strong opioids) and significant increases in strong opioid and antineuropathic prescriptions for patients in the last 3 months prior to a cancer-related death (IRR = 1.06, 95% CI: 1.04-1.07, p < 0.001 for strong opioids; IRR = 1.11, 95% CI: 1.08-1.14, p < 0.001 for antineuropathics). A spike in opioid prescriptions for patients diagnosed in Q2 2020 and those who died in Q2 2020 was observed and interpreted as stockpiling. More analgesics were prescribed in more deprived quintiles. This differential was less pronounced in patients towards the end of life, which we attribute to closer professional supervision.
Conclusions: We demonstrate significant changes to community analgesic prescriptions for cancer patients related to the UK pandemic and illustrate prescription patterns linked to patients' demographic background.
Keywords: Analgesia; COVID-19 pandemic; Cancer; Pain; Prescription; Primary care.
© 2023. The Author(s).
Conflict of interest statement
JH, FT, RG, SB, AA, BB, JL, GG, RT, TL, CA and DWH have nothing to declare. MR and RAL are members of the Welsh Government COVID-19 Technical Advisory Group. ML has received honoraria unrelated to this work from Bayer, Carnall Farrar, EMD Serono, Novartis, Pfizer and Roche.
Figures

References
-
- Society AC. Facts about cancer pain. 2019.
-
- World Health Organization . WHO guidelines for the pharmacological and radiotherapeutic management of cancer pain in adults and adolescents 2019. 2019. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
