

Trigeminal Nerve Involvement in Bulbar-Onset Anti-IgLON5 Disease
- PMID: 37607754
- PMCID: PMC10584367
- DOI: 10.1212/NXI.0000000000200153
Trigeminal Nerve Involvement in Bulbar-Onset Anti-IgLON5 Disease
Abstract
Objectives: Anti-IgLON5 disease (IgLON5-D) may present with a bulbar-onset motor neuron disease-like phenotype, mimicking bulbar-onset amyotrophic lateral sclerosis. Recognition of their distinctive clinical and paraclinical features may help for differential diagnosis. We report 2 cases of atypical trigeminal neuropathy in bulbar-onset IgLON5-D.
Methods: Trigeminal nerve involvement was assessed using comprehensive clinical, laboratory, electrophysiologic, and MRI workup.
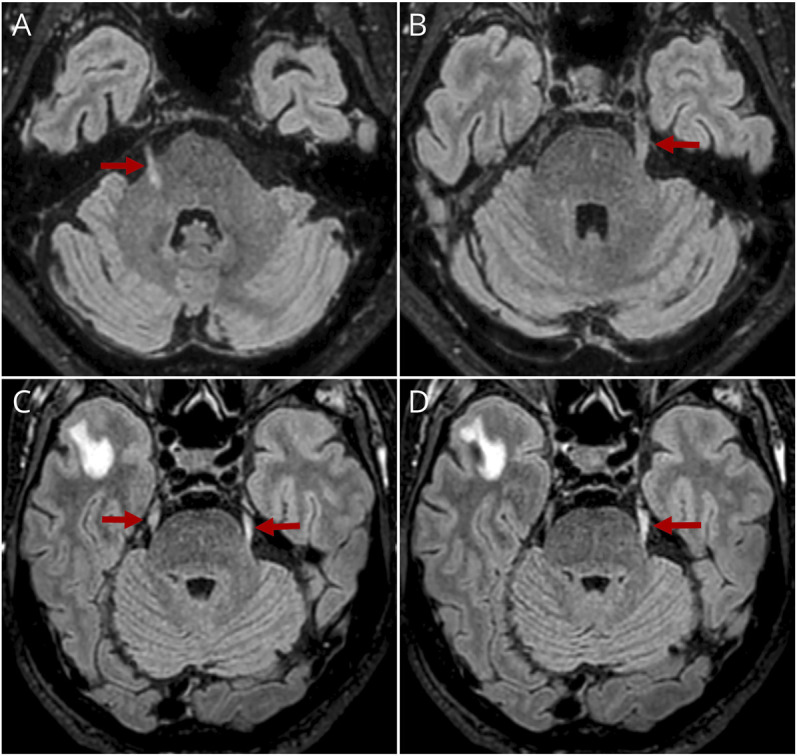
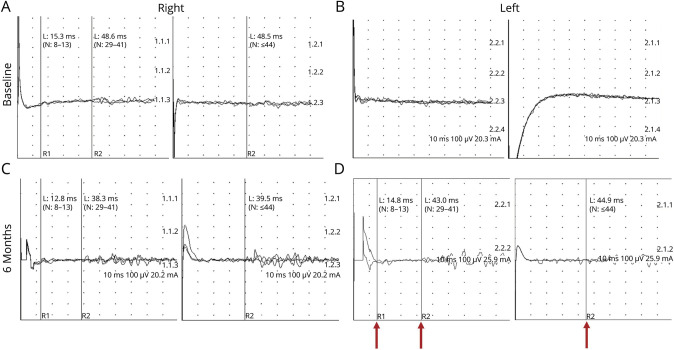
Results: Both patients were referred for progressive dysphagia, sialorrhea, and hoarseness. They were treated with bilevel positive airway pressure for nocturnal hypoventilation. Patient 1 complained of continuous facial burning pain with allodynia, exacerbated by mastication and prolonged speech. Patient 2 reported no facial pain. Anti-IgLON5 autoantibodies (IgLON5-Abs) were positive in serum for both patients and CSF for patient 1. Cerebral MRI revealed bilateral T2 fluid-attenuated inversion recovery (FLAIR) hyperintensity and enlargement of trigeminal nerves without gadolinium enhancement in both patients. Needle myography showed fasciculations in masseter muscles. Blink-reflex study confirmed bilateral trigeminal neuropathy only in patient 2. Cortical laser-evoked potentials showed a bilateral small-fiber dysfunction in the trigeminal nerve ophthalmic branch in patient 1.
Discussion: In case of progressive atypical bulbar symptoms, the presence of a trigeminal neuropathy or trigeminal nerve abnormalities on MRI should encourage the testing of IgLON5-Abs in serum and CSF.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures
References
-
- Sabater L, Gaig C, Gelpi Eet al. . A novel non-rapid-eye movement and rapid-eye-movement parasomnia with sleep breathing disorder associated with antibodies to IgLON5: a case series, characterisation of the antigen, and post-mortem study. Lancet Neurol. 2014;13(6):575-586. doi. 10.1016/S1474-4422(14)70051-1. Erratum in: Lancet Neurol. 2015;14(1):28. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical